- Case Report
- Open access
- Published:
Epiglottis calcification: forgotten cause of dysphagia in elderly population
Egyptian Journal of Radiology and Nuclear Medicine volume 55, Article number: 90 (2024)
Abstract
Background
Dysphagia is a relatively common clinical issue in elderly population with numerous causes, which are divided into oropharyngeal and substernal categories. Most of the causes of dysphagia can be diagnosed easily with clinical and radiological examinations. However, we encountered a rare cause of dysphagia in an elderly patient, which can be missed easily during diagnostic workup, that entity is epiglottis calcification.
Case presentation
A 91-year-old male presented with complaints of recurrent aspirations and difficulty in swallowing. Physical examination revealed no abnormalities in the oral cavity, pharynx and nose. Flexible fiberoptic laryngoscopic examination was performed, which mildly swollen and posteriorly moved epiglottis with limited mobility during swallowing. Computed tomography scan of the larynx revealed significant asymmetric amorphous calcification of the free edge of the aryepiglottic, pharyngoepiglottic, and epiglottis folds.
Conclusions
Although dysphagia is a common problem in elderly, it has serious complications such as recurrent aspirations, pneumonia and nutritional deficiency. One of the rare causes of dysphagia in elderly is epiglottic calcifications, which impairs its flexibility and the functionality, and may predispose to difficulty in swallowing and recurrent aspirations.
Background
Dysphagia is a relatively common clinical problem characterized by subjective feeling of obstruction or difficulty during deglutition. Causes of dysphagia can be divided into oropharyngeal and substernal. Oropharyngeal dysphagia can be caused by esophageal web, diverticula, tumors or extrinsic compression such as multinodular goiter and retropharyngeal abscess [1]. One of rare causes of oropharyngeal dysphagia is epiglottic calcification and resultant abnormal movement of epiglottis, thus predisposing patient to recurrent aspirations [2]. In this report, we are going to discuss a case of epiglottis calcification in an elderly patient, leading to complaints of dysphagia and recurrent aspirations.
Case presentation
-
a.
Clinical history. A 91-year-old male presented with complaints of recurrent aspirations and difficulty in swallowing. Patient had these complaints for approximately 2 years with gradual progression in the last few months. He had no history of neck pain, snoring, dysphonia, dyspnea, or any other symptoms. No previous history of significant weight loss, smoking, drug usage, symptoms associated with gastroesophageal reflux disease was present. History of systemic illnesses such as diabetes or hypertension was not present. No previous history of any malignancy was present.
-
b.
Physical examination. Patients’ physical examination revealed no abnormalities in the oral cavity, pharynx and nose. The patient's evaluation by the gastrointestinal and internal medicine departments did not reveal any additional reason for the amorphous calcification of the epiglottis or dysphagia. The patient's blood levels of calcium, phosphorus and parathyroid hormone were normal.
-
c.
Endoscopic findings. Flexible fiberoptic laryngoscopic examination was performed, which mildly swollen and posteriorly moved epiglottis with limited mobility during swallowing. Stasis was noted in the pyriform sinuses with free edge of epiglottis being forced in the direction of the pharynx's rear wall. Both the actual and false vocal chords examined were normal.
Upper gastrointestinal endoscopy shows no significant abnormality.
-
d.
Imaging findings. Further, to determine the etiology and make sure a mass lesion was not missed, a computed tomography (CT) scan of the larynx was conducted with axial, coronal and sagittal reformat. It revealed significant asymmetric amorphous calcification of the free edge of the aryepiglottic, pharyngoepiglottic and epiglottis folds (Figs. 1, 2, 3). No definite solid mass lesion noted in oral cavity, pharynx, larynx and neck regions.
Fig. 1 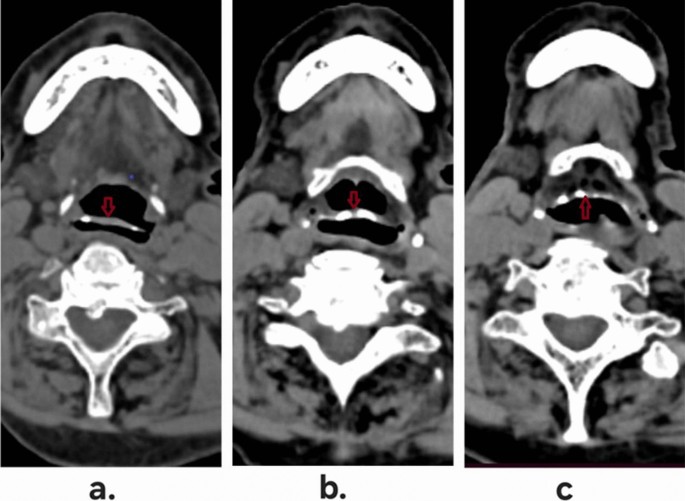
Axial images of CT scan of neck region, showing free edge (a), mid-region (b) and inferior fixed part (c) of the epiglottis, showing multifocal coarse calcification (red arrow)
Fig. 2 
Sagittal images of CT scan of neck region, showing right lateral (a), midline (b) and left lateral (c) parts of the epiglottis, showing multifocal coarse calcification (green arrow)
Fig. 3 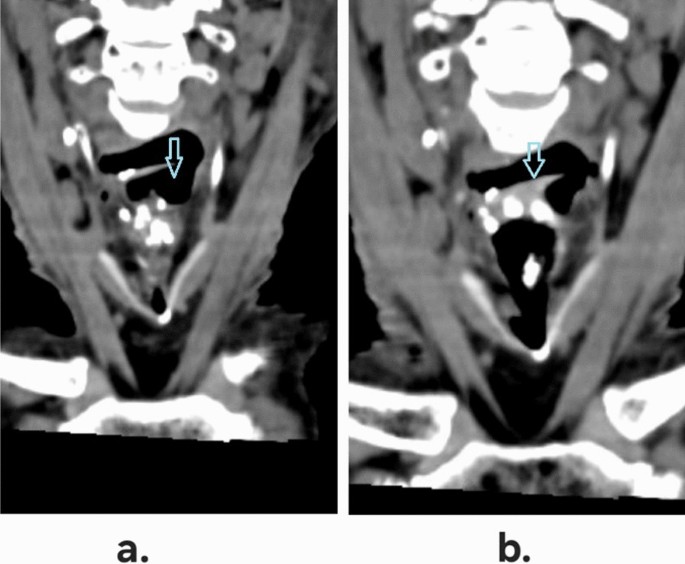
Coronal images of CT scan of neck region, showing anterior (a) and posterior (b) sections of the epiglottis, showing extensive amorphous cartilaginous calcification (blue arrow)
Barium swallow shows no significant abnormality in both pharyngeal and esophageal phases (Fig. 4).
Fig. 4 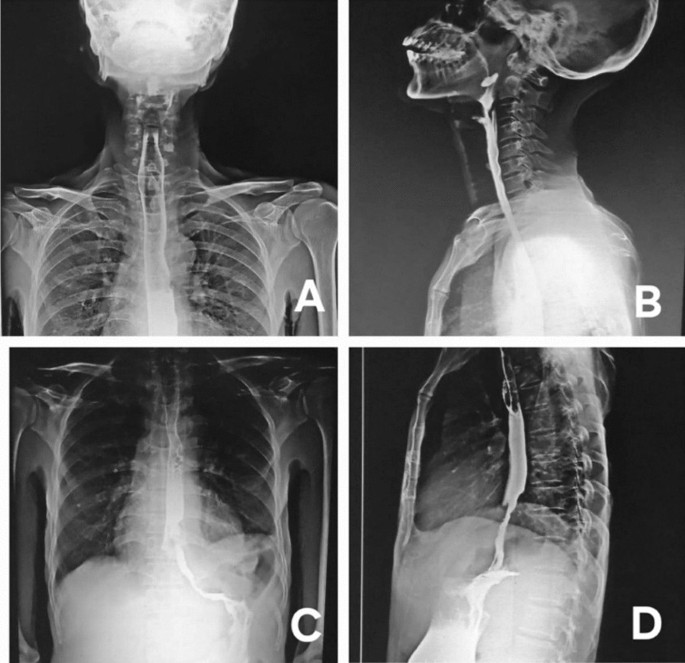
Barium swallow images—pharyngeal phase anteroposterior (A) and lateral (B) projections, as well as esophageal phase anteroposterior (C) and lateral (D) projections. No any obstructive lesion or stenotic pathology noted in the images
-
e.
Clinical advice and follow-up. During examination, otorhinolaryngologist found that the patients complain of difficulty in swallowing is reduced with slight flexion of his head. Patient was advised to take short meals at frequent interval with slight flexion of head. Further, patient had been advised for 3 monthly follow-up visits to assess the symptomatic relief and progression of disease, if any.




Discussion
Dysphagia has high prevalence of in older adults and is associated with serious consequences; hence, it is considered as a separate geriatric entity [3]. Causes of dysphagia are divided into oropharyngeal and esophageal categories. Common causes of oropharyngeal dysphagia in elderly include progressive neurologic diseases such as dementia, parkinsonism, head and neck cancers, and stroke. Similarly, common causes of esophageal dysphagia in such population are esophageal strictures, esophagitis and achalasia [3].
Causes of dysphagia can also be categorized into mechanical ones and neuromuscular (motor) ones. Mechanical reasons of esophageal dysphagia (like tumor or stricture) initially cause difficulty in swallowing solid foods, and with time, it progresses to dysphagia with liquid foods also. If esophageal dysphagia is happening with both solid and liquid foods from the beginning itself, it most likely suggests a neuromuscular (motor) etiology, such as achalasia [4]. Detailed clinical history is helpful in such conditions to narrow down the differentials and in guiding the appropriate workup [5].
One of the rare and often overlooked causes of dysphagia in elderly population is calcification of epiglottis (chondrocalcinosis) [6]. Epiglottis consists of elastic cartilage, and such cartilages rarely show any tendency for calcification, and hence, it is very rare for epiglottis to show significant coarse or radiologically visible calcification [6]. But such cases have been reported in the literature [2, 3, 6].
Epiglottis usually does not calcify similar to laryngeal cartilages, owing to its elastic nature; however, calcium deposition in epiglottis elastic cartilage increases with age, as showed by Kano et al. [7].
Calcification of epiglottis may result in its movement abnormalities and may lead to dysphagia and various swallowing and aspiration problems. The epiglottis is a leaf-shaped flap of cartilage tissue and is important in preventing the aspiration of liquid or solid foods during swallowing [6]. It is mainly composed of elastic cartilage which provides it flexibility and thus helpful in its dynamic function. Patterns of abnormal epiglottic movement such as translocation, immobility and horizontal tilt may lead to difficult swallowing and loss of coordination during deglutition, leading to recurrent aspirations [7].
The epiglottis and other laryngeal cartilages, such as the cuneiform and the corniculate, are made of yellow elastic fibro cartilage, which may calcify progressively with age. Apart from calcification due to natural aging, other causes of epiglottis calcification are radiotherapy, granulomatous disease, or as sequelae to secondary hyperparathyroidism [2]. Our case demonstrates epiglottic cartilage calcification without identified cause.
Similar cases have also been reported by Günbey et al. [2] and Fernández-Rodríguez et al. [6]. Both these cases showed age-related coarse epiglottis calcification in elderly patients, without any identifiable causes. Günbey et al. [2] also reported the movement abnormality in epiglottis due to its calcification as a cause of dysphagia.
Epiglottis covers across the laryngeal inlet and hence prevents aspiration of contents. Calcification of epiglottis cartilages alters its mechanical properties and can obstruct the food passage through pharynx. It also exposes patient to recurrent aspirations and risk of pneumonia [2].
Hence in cases of dysphagia, particularly in elderly population, where no cause can be pinpointed for it, epiglottis must be assessed for calcification and the resultant movement abnormality [8].
Most of the cases of epiglottis calcification with dysphagia are treated conservatively, with emphasis on symptomatic relief. Finding the best possible positioning of head and neck during swallowing allows relief in dysphagia. In cases where conservative management fails to provide relief, surgical procedures such as supraglottoplasty or epiglottopexy should be considered [9, 10].
Conclusions
Although dysphagia is a common problem in elderly, it has serious complications such as recurrent aspirations, pneumonia and nutritional deficiency. It can have many causes, both common and rare ones. One of the rare causes of dysphagia in elderly is epiglottic calcification. Epiglottis calcification impairs its flexibility and thus functionality and may predispose to difficulty in swallowing and recurrent aspirations. Although epiglottis calcification can easily be diagnosed on CT study of neck, but it can easily be overlooked without a grade of suspicion. Epiglottic calcification is still a diagnosis of exclusion when no other cause for dysphagia in elderly could be reached after clinical examinations and radiological investigations. Hence, for radiologists, it is helpful to remember this entity and to check in scans for dysphagia, especially, when no other imaging explanation for dysphagia is found.
Availability of data and materials
The data and images in the current study are available from the corresponding author, on reasonable request.
Abbreviations
- CT:
-
Computed tomography
References
Kuo P, Holloway RH, Nguyen NQ (2012) Current and future techniques in the evaluation of dysphagia. J Gastroenterol Hepatol 27:873–881. https://doi.org/10.1111/j.1440-1746.2012.07097.x
Günbey HP, Günbey E, Sayit AT (2014) A rare cause of abnormal epiglottic mobility and dyspagia: calcification of the epiglottis. J Craniofacial Surg 25(6):e519–e521. https://doi.org/10.1097/SCS.0000000000001025
Baijens LW, Clavé P, Cras P et al (2016) European Society for Swallowing Disorders—European Union Geriatric Medicine Society white paper: oropharyngeal dysphagia as a geriatric syndrome. Clin Interv Aging 11:1403–1428. https://doi.org/10.2147/CIA.S107750
Marik PE, Kaplan D (2003) Aspiration pneumonia and dysphagia in the elderly. Chest 124:328–336. https://doi.org/10.1378/chest.124.1.328
O’Horo JC, Rogus-Pulia N, Garcia-Arguello L et al (2015) Bedside diagnosis of dysphagia: a systematic review. J Hosp Med 10(4):256–265
Fernández-Rodríguez A, Benito-Orejas JI, Jiménez-Pérez AE et al (2009) Calcification of the epiglottis. Acta Otorrinolaringol Esp 60:215–216. https://doi.org/10.1016/s0001-6519(09)71236-1
Kano M, Shimizu Y, Okayama K et al (2005) A morphometric study of age-related changes in adult human epiglottis using quantitative digital analysis of cartilage calcification. Cells Tissues Organs 180:126–137. https://doi.org/10.1159/000086753
Garon BR, Huang Z, Hommeyer M et al (2002) Epiglottic dysfunction: abnormal epiglottic movement patterns. Dysphagia 17:57–68. https://doi.org/10.1007/s00455-001-0102-8
Diaz S, Ekberg O (2010) The frequency of diagnostic errors in radiologic reports depends on the patient’s age. Acta Radiol 51:934–938. https://doi.org/10.3109/02841851.2010.503192
Okuyama Y, Nonomura Y, Hatanaka N (2000) A patient with dysphagia treated successfully and is charged without nutritional support. Gan To Kagaku Ryoho 27:754–755
Acknowledgements
Not applicable.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
Patient selection and follow-up were done by NS and DV. The manuscript was written by NS, SV and DV. All the authors have made necessary comments and contributions to the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The procedure described was in accordance with the institutional ethical guidelines and conform to the WMA Declaration of Helsinki—Ethical principles for medical research involving human subjects.
Consent for publication
Written informed consent was obtained from the patient and patient relatives for publication of the article.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Seth, N., Varshney, D. & Verma, S. Epiglottis calcification: forgotten cause of dysphagia in elderly population. Egypt J Radiol Nucl Med 55, 90 (2024). https://doi.org/10.1186/s43055-024-01264-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01264-5