- Research
- Open access
- Published:
CSF rhinorrhea: non-contrast CT, contrast-enhanced CT cisternography or combined?
Egyptian Journal of Radiology and Nuclear Medicine volume 53, Article number: 201 (2022)
Abstract
Background
Radiologic diagnosis of CSF leaks is challenging. We evaluated the diagnostic value of non-contrast CT and contrast-enhanced CT cisternography in identifying the presence of CSF rhinorrhea and site of leak as well as comparing them to surgical data and/or clinical follow-up.
Results
Fifty patients (20 males and 30 females) were included in our study with age ranging from 19 to 67 years. 76% of cases had spontaneous CSF rhinorrhea. Cribriform plate defect was the most common site of CSF leak, accounting for about 50% of cases. The highest sensitivity, specificity, PPV and NPV for diagnosis of CSF rhinorrhea were observed with the combined NCCT and CECTC with values 87%, 100%, 100% and 67%, respectively.
Conclusion
Accurate surgical planning and successful dural repair requires accurate localization of the dural and osseous defects. CT cisternography which already involves pre-cisternography non-contrast images holds great sensitivity in detection of the exact defect site together with confirmation of the CSF leak.
Background
CSF rhinorrhea is defined as passage of CSF from the subarachnoid space through the osseous and dural defect at skull base into the nasal cavity [1].
Causes of CSF rhinorrhea can be generally classified into traumatic (including iatrogenic) and non-traumatic; the non-traumatic causes include tumors and spontaneous leaks [2].
The patients may be presented by a wide variety of symptoms including clear nasal discharge and headache or develop complications like meningitis, pneumocephalus or even brain abscess [3] that is why closing the defect, either endoscopic or surgical, is of paramount importance which in turn requires accurate localization of its site and measurement of its dimensions [2].
CSF rhinorrhea can be divided into active when continuous dripping is encountered or inactive when the dripping is intermittent [3].
Different imaging modalities including isotope scans, computed tomography (CT) and magnetic resonance (MR) imaging techniques have been employed to localize and characterize skull base defects that are believed to be responsible for CSF leakage. Yet, there is no gold standard imaging modality [3].
High-resolution computed tomography (HRCT) provides accurate bony details, but it is difficult to differentiate paranasal sinus secretions from leaked CSF. While contrast-enhancing CT cisternography has the advantage of crucial proof of CSF leak in addition to the definitive anatomical localization of the osseous defect, major side effects including headache, meningeal irritation and seizures may occur [4].
Unlike CT cisternography, MR cisternography does not demand an active CSF leak to demonstrate the site of leak. Inactive leaks are often under-diagnosed on CT cisternography, but CT imaging is still superior in assessment of osseous anatomy [4].
Radionuclide cisternography is seldom performed nowadays; active CSF leakage should be present at the time of examination for accurate diagnosis, whereas intermittent CSF leaks require a prolonged cisternography with a radiotracer having a longer biological half‑life. It also does not provide exact anatomic localization of CSF leaks [4, 5].
Methods
Fifty patients presented by CSF rhinorrhea were included in the study, 20 males and 30 females with age ranging from 19 to 67 years, from May 2019 to November 2021, after ethical committee approval and patient’s consent. All scans were obtained using Siemens Somatom Perspective 128-row Multidetector Scanner. The scanning parameters were done with automated tube current modulation (mA); 110 kVp; pitch 1.5; rotation time 1.0 s; and gantry angle zero. The reconstruction parameters were adjusted as follows: helical thickness 1 mm; standard and bone reconstruction was used. Non-contrast high-resolution CT was obtained in a supine position from the level of skull vault to the mandible followed by intrathecal injection of 20 cm of Omnipaque (300 mg/ml) through lumbar puncture. All patients were thereafter placed with the head in the dependent position in the prone kneeling position for 10 min to facilitate opacification of the cisterns followed by CT in prone position. After that, studies were transferred to workstation for interpretation of the acquired images in multiplanar reformatting. Non-contrast CT studies were assessed independently to determine the presence of bone defects, and contrast-enhanced CT cisternography examinations were then reviewed and compared with the non-contrast images. The anatomical location of the defect and its size were recorded in 30 cases. The anatomical location of the contrast leakage without visualization of the defects was recorded in 8 cases.
Out of the 50 patients, only 29 underwent surgical repair of their CSF leak. The operative reports for these patients were reviewed and compared to the imaging data.
Statistical analysis of the present study was conducted by SPSS V.20. Qualitative data were presented using number and percentage. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of NCCT and CECTC were calculated in order to conclude the diagnostic value of each modality and their combination with the operative and clinical follow-up taken as the gold standard.
Results
Fifty patients were included in the current study, 20 males and 30 females with age ranging from 19 to 67 years. All these 50 patients presented with watery discharge from nose (rhinorrhea) (27 of them from the left side and 23 from the right side).
Thirty-eight cases showed spontaneous CSF rhinorrhea, while 9 patients had a history of trauma and only 3 patients had a history of previous surgeries, two of them underwent endoscopic paranasal surgery and one underwent trans-sphenoidal neurosurgery (Table 1).
Out of the 50 patients included in this study, 12 showed no bone defect in non-contrast CT (NCCT) nor CSF leak in contrast-enhanced CT cisternography (CECTC) in spite of history of CSF leak (24% of cases). Ten of these patients showed clinical resolution of symptoms after medical treatment and did not undergo subsequent imaging or intervention, while two patients had persistent symptoms that required endoscopic intervention. Bone defects and/or CSF leak were identified in the remaining 38 patients, accounting for 76% of the study group.
Out of the 38 patients with visualized bone defects and/or CSF leak, 26 patients had spontaneous rhinorrhea with no traumatic or surgical history.
The site of bone defect and/or CSF leak of a total of 38 patients are shown in Table 2.
The defects ranged in size from 0.6 to 8 mm, with an average size of 4.2 mm.
Twenty-nine of 38 patients with bone defects and/or CSF leak underwent surgical exploration and repair, seven patients experienced clinical resolution of CSF leak, and two sought treatment elsewhere or were lost to follow-up.
Out of these 29 patients with confirmed bone defects and/or CSF leak by surgery, 19 patients showed bone defect in NCCT and CSF leak in contrast-enhanced CT cisternography (CECTC), while 7 patients showed contrast leak on CECTC with no sizeable defect in NCCT and only 3 patients showed bone defect in NCCT but no CSF leak in CECTC.
Out of the 7 patients, that showed positive results in CT and responded to medical treatment without the need for surgical intervention, 6 patients showed both bone defect in NCCT and CSF leak in CECTC, while only 1 patient showed contrast leak on CECTC with no sizeable defect in NCCT.
The overall sensitivity, specificity, positive predictive value and negative predictive value of a total of 48 patients (only two patients were excluded, who sought treatment elsewhere or were lost to follow-up) regarding combined NCCT and CECTC, as well as of each method separately, are shown in Table 3.
Cases
- Case 1:
-
Female patient aged 60 years old, presented with right-sided CSF rhinorrhea, CT showed contrast leak through a defect at the roof of right sphenoid sinus measuring 3 mm (Fig. 1).
Fig. 1 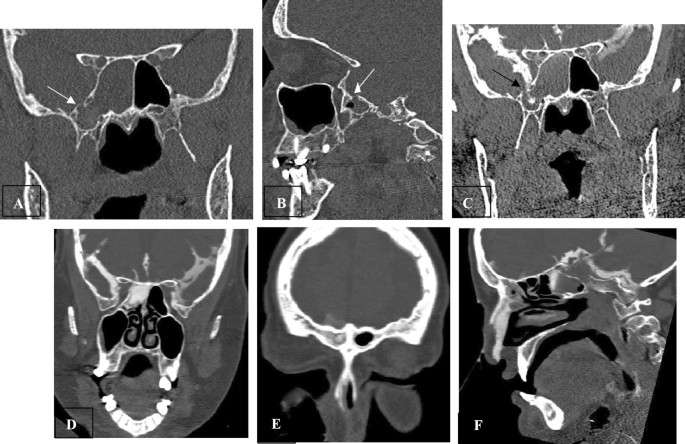
Non-contrast CT with bone window in coronal and sagittal planes (A and B) show bony defect (3 mm) at roof of right compartment of sphenoid sinus (white arrow), CT cisternography in coronal plane (C) show CSF active contrast leak through that bony defect (black arrow) into the right sphenoid sinus (D), right frontal sinus (E) and right nasal cavity (F)
- Case 2:
-
Female patient aged 38 years old with a history of previous endoscopic sinus surgery and turbinectomy (Fig. 2).
Fig. 2 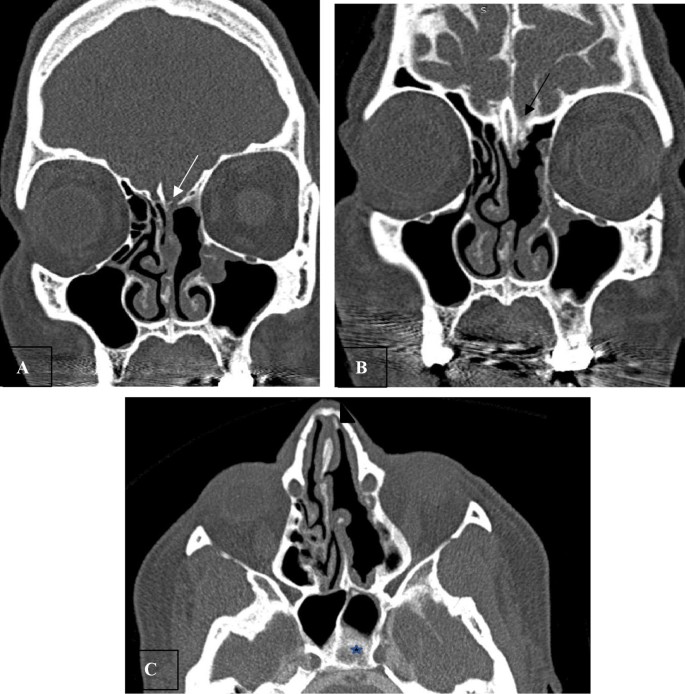
Non-contrast CT in coronal plane (A) shows defect in left cribriform plate of ethmoid (white arrow), CT cisternography in coronal and axial planes (B&C) show: contrast leak through left cribriform plate of ethmoid (black arrow) (B) to the left nasal cavity and left sphenoid sinus (arrowhead and star) (C). Note previous left middle turbinectomy, partial excision of nasal septum, minimal mucosal thickening of both maxillary sinuses and mildly deviated nasal septum to the right side (A and B)
- Case 3:
-
Female patient aged 25 years old, presented with right-sided nasal watery discharge (CSF rhinorrhea) (Fig. 3).
Fig. 3 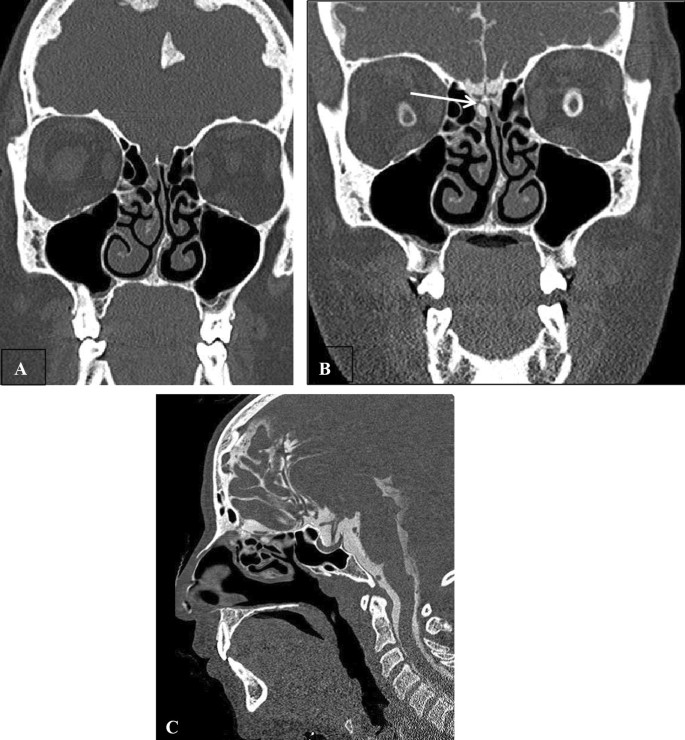
Non-contrast CT with bone window in coronal plane (A) shows no bone defect, CT cisternography in coronal and sagittal planes (B and C, respectively) show: CSF contrast leak into the right ethmoidal sinus (white arrow). Note mild bilateral mucosal thickening of both maxillary sinuses, left nasal septum spur and mildly deviated nasal septum to the left side
- Case 4:
-
Male patient aged 42 years old with right-sided CSF rhinorrhea (Fig. 4).
Fig. 4 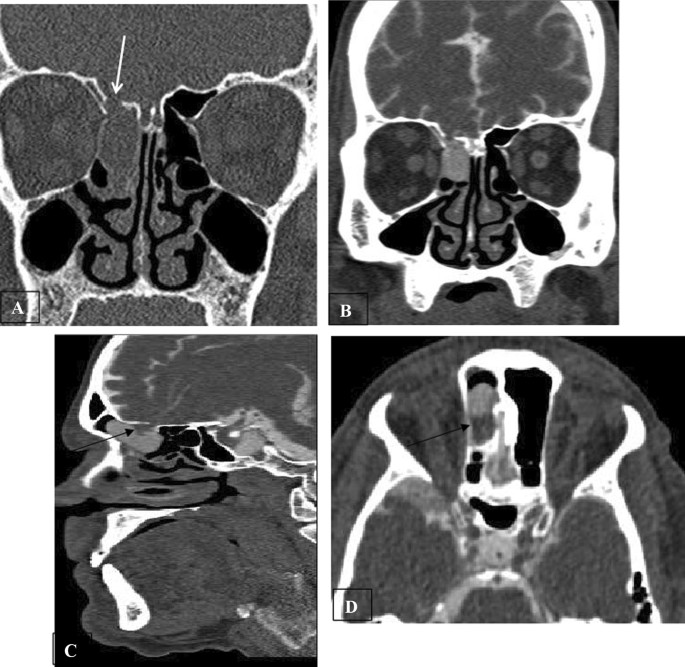
Non-contrast CT in coronal (A), CT cisternography in coronal (B), sagittal (C) and axial (D) planes show defect measuring 6 mm in the roof of the right ethmoid sinus (white arrow) (A and B) with evidence of contrast leak through this defect in addition to herniated brain tissue from the right frontal lobe (black arrow) (C and D)




Discussion
A cranial CSF leak or fistula is defined as a loss of CSF from the intracranial cavity resulting from an osseous defect in the skull base. It is related to disruption of the dura and arachnoid mater, leading to communication between the intracranial and nasal cavities [6]
Imaging plays a remarkable role in preoperative workup through localizing the site of the leak and determining the accurate dimensions of the osteodural defect [7]. However, there is no imaging “gold standard” for diagnosis of such important entity reflecting the difficulty of this diagnosis [3].
In our study, the most common cause of CSF rhinorrhea was spontaneous leakage; this is in agreement with Shetty et al. [8]. On the other hand, Yilmazlar et al. [9] reported that traumatic etiology was the most common cause. This is attributed to the selection of patients with a history of head injury in Yilmazlar et al. study population.
Twelve patients (24%) had normal imaging findings, ten of them experienced resolution of their CSF leak; this is comparable to Stone et al. [5], who stated that 28% of cases showed no bone defects or contrast leak. It is possible that the bone defects in these patients were tiny with inactive leakage in which the dripping is intermittent.
Our results showed that the most common site of the bony defect is the cribriform plate (50%) which is in line with Atta et al. [3], where 40% of their cases showed bone defects at cribriform plate, whereas Scholsem et al. [10] found a high percentage of leaks through cribriform plate (87%).
Our study stated that NCCT detected bone defects in 30 cases (75%), while CECTC detected contrast leak in 35 cases (87.5%); this is against Lupo et al. [11], who stated that 100% of bony defects could be detected by NCCT, while 84.6% only of cases showed contrast leak in CECTC; this may be attributed to small sample size in their study; also in our study, nearly 50% of cases showed defect at cribriform plate, which is a sieve-like structure and is normally perforated by olfactory nerve. On the other side, our results were comparable with stone et al. as regards NCCT defect detection which was 71%, while no added cases by CECTC in that study, which disagreed with our study that added 5 more cases [5].
Our results showed that NCCT showed a sensitivity of 74%; this is lower than Shetty et al. [8] who showed a sensitivity of 92% but both studies showed the same specificity of 100%.
Our results showed that CECTC showed a sensitivity of 87%; this is relatively higher than Eberhardt et al. [12], who stated that its sensitivity equals 72.3%.
We consider that the greatest advantage of NCCT added to CECTC is precise anatomical localization of the osseous defect with definitive proof of CSF leak. This was confirmed by results in the current study which showed higher sensitivity of combined NCCT and CECTC of 95% and specificity of 100%, compared to either modality alone.
Conclusion
CT cisternography is very useful in evaluation of patients with CSF leak. Combined non-contrast images and CT cisternography showed higher sensitivity in detection of the site of CSF leakage and thus help in proper treatment planning. Although large defects can be easily visualized on NCCT, small defects mostly require CECTC to visualize the contrast leak.
Availability of data and materials
The authors confirm that all data supporting the finding of the study are available within the article, and the raw data and data supporting the findings were generated and available at the corresponding author on request.
Abbreviations
- CSF:
-
Cerebrospinal fluid
- CT:
-
Computed tomography
- NCCT:
-
Non-contrast CT
- CECTC:
-
Contrast-enhanced CT cisternography
- MR:
-
Magnetic resonance
- HRCT:
-
High-resolution computed tomography
- PPV:
-
Positive predictive value
- NPV:
-
Negative predictive value
References
Rahalkar MD, Rahalkar AM, Joshi VS, Sant KV, Zade KB (2018) Computed tomography cisternography for the management of cerebrospinal fluid fistulae. Int J Otorhinolaryngol Clin 10(1):17–27
Scoffings DJ (2021) Imaging of acquired skull base cerebrospinal fluid leaks. Neuroimaging Clin N Am 31(4):509–522
Atta H, Seifeldein G, Almamoun M, Imam H (2017) Reliability of multidetector CT in the diagnosis of cerebrospinal fluid rhinorrhea with operative correlation. Egypt J Radiol Nuclear Med 48(1):107–113
Vemuri NV, Karanam LS, Manchikanti V, Dandamudi S, Puvvada SK, Vemuri VK (2017) Imaging review of cerebrospinal fluid leaks. Indian J Radiol Imaging 27(4):441446
Stone JA, Castillo M, Neelon B, Mukherji SK (1999) Evaluation of CSF leaks: highresolution CT compared with contrast-enhanced CT and radionuclide cisternography. AJNR Am J Neuroradiol 20(4):706–712
Lloyd KM, DelGaudio JM, Hudgins PA (2008) Imaging of skull base cerebrospinal fluid leaks in adults. Radiology 248(3):725–736
Hiremath SB, Gautam AA, Sasindran V, Therakathu J, Benjamin G (2019) Cerebrospinal fluid rhinorrhea and otorrhea: a multimodality imaging approach. Diagn Interv Imaging 100(1):3–15
Shetty PG, Shroff MM, Sahani DV, Kirtane MV (1998) Evaluation of high resolution CT and MR cisternography in the diagnosis of cerebrospinal fluid fistula. AJNR Am J Neuroradiol 19:633–639
Yilmazlar S, Arslan E, Kocaeli H, Dogan S, Aksoy K, Korfali E et al (2006) Cerebrospinal fluid leakage complicating skull base fractures: analysis of 81 cases. Neurosurg Rev 29:64–71
Scholsem M, Scholtes F, Collignon F, Robe P, Dubuisson A, Kaschten B et al (2008) Surgical management of anterior cranial base fractures with cerebrospinal fluid fistulae: a single-institution experience. Neurosurgery 62(2):463–471
Lupo FA, Perfetto SC, Sticchi G, Perrone A (2000) Comparative study of CTCisternography, high resolution CT and MR cisternography in Rhinorrhoea. Riv Neuroradiol 13(5):703–710
Eberhardt KE, Hollenbach HP, Deimling M, Tomandl BF, Huk WJ (1997) MR cisternography: a new method for the diagnosis of CSF fistulae. Science 7(9):1485–1491
Acknowledgements
The authors thank all the participants for their cooperation and patience.
Funding
No funding. Not applicable for this section.
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript for submission. AA suggested the research idea, ensured the original figures and data in the work, minimized the obstacles to the team of work, correlated the study concept and design and had the major role in analysis. LH collected data in all stages of manuscript and performed data analysis. RE supervised the study with significant contribution to design the methodology, manuscript revision and preparation. LH and RE correlated the clinical data of patient and matched it with the findings, drafted and revised the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed written consents were obtained from the patients; the study was approved by ethical committee of Tanta University Hospital, Faculty of Medicine.
Consent for publication
All participants included in the research gave written consent to publish the data included in the study. The authors accepted to publish the paper.
Competing of interests
The authors declare that they have no competing of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hablas, L.T., Ammar, A.M. & Elnagar, R.M. CSF rhinorrhea: non-contrast CT, contrast-enhanced CT cisternography or combined?. Egypt J Radiol Nucl Med 53, 201 (2022). https://doi.org/10.1186/s43055-022-00889-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00889-8