- Review
- Open access
- Published:
Differential diagnoses of cavitary lung lesions on computed tomography: a pictorial essay
Egyptian Journal of Radiology and Nuclear Medicine volume 54, Article number: 149 (2023)
Abstract
Background
Cavitary lung lesions are frequent findings on imaging, with the most common sources being malignancies and infections. They have multiple etiologies and differential diagnoses, which can have overlapping imaging characteristics, posing a diagnostic difficulty.
Main body of the abstract
This article is an educational pictorial essay highlighting the pitfalls and differential diagnoses of lung cavities, and focusing on the typical imaging patterns, the clinical and biological contexts of each etiology, illustrated by images that were extracted from the images archiving system of our radiology department.
Short conclusion
The radiologist should be aware of all etiologies of cavitary lung lesions, including the less frequent ones, and be familiar with their imaging patterns and characteristics, which aids in establishing the diagnosis or, at the very least, narrowing down the evoked diagnoses.
Background
A lung cavity is defined as a lung lesion containing gas and surrounded by a wall of a variable thickness [1].
An excavation is defined as the appearance of a cavity, which can be inside of an opacity (Consolidation, mass, or nodule) [1].
Different mechanisms can lead to formation of cavities; the most common one is loss of substance by necrosis inside of a mass or nodule, which may be neoplastic, infectious, or ischemic. The necrotic material will be evacuated totally or partially by a bronchus and replaced by air. Other mechanisms encompass a mechanical loss of substance without necrosis (e.g., trauma.), and cystic malformation [1].
Computed tomography (CT) scan is a more accurate diagnostic tool in comparison with conventional radiography, allowing the detection and analysis of cavitary lesions, even when they are small, and specifying, in a more sensitive way, the characteristics of lesions and the presence or absence of associated lesions. Moreover, it also allows CT-guided biopsies for suspicious cases [2].
The purpose of this article is to review the pathologies that give rise to cavitary lung lesions that radiologists encounter in their daily practice. These have been categorized into two main groups: frequent etiologies and rare etiologies.
Main text
Imaging features to analyze in a cavity
The wall
-
Thickness:
Maximal thickness is a very informing characteristic:
A thickness above 4 mm is considered thick, and a thickness below 4mm is considered thin. Thin-walled cavities below 2 mm can be called cysts [3].
In solitary cavities, a thickness below 4 mm is highly suggestive of benignity (92% are benign), a thickness between 4 and 15 mm reflects a moderate risk of malignancy (49% are malignant), and a thickness over 15 mm is very suggestive of malignancy (95% are malignant).
-
Margins: Can be smooth and regular or irregular. Malignant lesions are associated with irregular inner and outer margins [4].
Content
The content could be totally air, or partially air (mixed; solid and or liquid content, in addition to air).
The liquid component could be due to blood, pus, bronchial secretions, or liquefied necrosis, causing a horizontal air–liquid level.
The solid component could be tumoral, fungal, blood clot, sequestrum, or pus [1].
Other features to analyze
-
Size: The size is especially valuable for follow-up and assessing treatment response.
-
Number: Single or multiple (e.g., metastases tend to be multiple).
-
Topography and distribution: Unilateral or bilateral, diffuse or predominant in a certain region (the periphery, the perihilum, the upper regions or the lower regions) (e.g., Tuberculosis typically affects the upper regions) [5].
-
Evolution: Comparing the current CT findings with the prior CT findings allows the distinction between:
-
An opacity that underwent excavation.
-
An ancient cavity that filled with liquid (infection of the cavity).
-
An ancient cavity that filled with solid content (aspergillus colonization of a residual cavity, for example) [6].
-
Associated lesions: Pulmonary, mediastinal, pleural, or distant associated lesions (Bone, liver, adrenal glands…).
Differential diagnoses
Pseudo-cavities
Pulmonary emphysema
It shouldn’t be considered a cavity as it has no wall. On imaging, a pseudo-wall of 1mm thickness can be seen as a result of compressed and piled up parenchymal septa around the emphysema (Fig. 1). Vessels can be seen within the center of the emphysema [7].

Axial CT image of the chest in the lung window of a 50-year-old male, showing multiple paraseptal and centrilobular emphysemas. Notice the absence of a wall. Only piled up septa around can be seen as pseudo-walls
Emphysema can be infected and manifest an air-fluid level (Fig. 2).

Axial CT image of the chest in the lung window of a 70-year-old male, showing an infected emphysema containing an air-fluid level in the left apex of the lung
Cystic bronchiectasis
It is a dilated bronchus characterized with a saccular “pouch-like” ending. What distinguishes them from cavities is the presence of bronchial systematization. They align in a hilo-peripheral axis, or group together in the para-mediastinum area creating a “cluster of grapes” appearance (Fig. 3) [1, 8].

Axial CT image of the chest in the lung window of a 55-year-old male, showing bilateral cystic bronchiectasis in the lower lobes of the lung (with mucoid impactions in this case)
Honeycombing
Honeycombing is a group of clustered small pulmonary cyst-like lesions, generally between 3 and 10 mm in diameter, arranged in multilayers, most commonly in the subpleural space (Fig. 4). This appearance is due to parenchymal destruction and retraction surrounded by fibrotic walls, as a consequence of fibrotic changes [9].This clarifies why they are categorized as pseudo-cavities.

Axial CT image of the chest in the lung window of a 67-year-old male, showing honeycomb cysts keeping with fibrosis
Diaphragmatic hernia
Diaphragmatic hernia can be congenital or acquired (iatrogenic or traumatic), it occurs through a diaphragmatic defect or through a weakened diaphragmatic hiatus.
Herniated intestinal loops or stomach could look similar to cavitary lesions on axial slices, but on coronal and sagittal reconstructions, the continuity to the abdominal cavity through the diaphragm is easily seen along with the collar sign at the level of the diaphragm (Fig. 5). The diaphragmatic defect (discontinuity) is sometimes visible [10, 11].

CT images of the chest in the lung window of a 49-year-old female, in the axial (A) and the coronal (B) planes, showing a herniation of the stomach and the peritoneal fat in the right hemithorax. Note its continuity toward the abdominal cavity and the collar sign (arrows) at the level of the diaphragm visible on the coronal plane
Extra-pulmonary cavities
Pleural empyema is a differential diagnosis for peripheral lung abscess.
A pleural empyema tends to be oval in shape, forms an obtuse angle with the chest wall, and has regular and fine margins. It compresses the adjacent parenchyma (including bronchi and vessels) and separates the visceral and parietal pleura (split pleural sign) (Fig. 6) [12].

Axial post-contrast CT image of the chest in the mediastinal window of a 26-year-old female, showing a right pleural empyema with air bubbles within, and an enhancement and thickening of the pleura
Frequent etiologies
Infectious
Tuberculosis
Tuberculosis is a bacterial infection due to Mycobacterium Tuberculosis, in the clinical context of tuberculosis contagion, subacute or chronic cough, nocturnal sweats, and anorexia.
Tuberculous lung cavities are present in 45% of post-primary tuberculosis and is less frequent in primary infection.
Cavitation is due to caseous necrosis and is located most frequently in the apical and posterior segments of upper lobes, and the superior segments of lower lobes (Fowler).
It appears on CT as a lesion with total air content (it seldom has an air–liquid level), and with a thick irregular wall.
An active tuberculosis is typically associated with centrilobular micronodules and consolidation (Fig. 7). It can also be accompanied with lymphadenopathies [13, 14].

Axial CT image of the chest in the lung window of a 17-year-old male, showing a cavitary lesion in the right Fowler segment, associated with diffuse and bilateral tree in bud micronodules, in a patient with active tuberculosis
Pulmonary abscess
A pulmonary abscess is a cavity filled with pus developed in a pneumonia site. It is associated with clinical and biological infectious signs.
It is often caused by Klebsiella Pneumoniae, Pseudomonas Aeruginosa, or anaerobic organisms.
Rupture of the abscess and the evacuation of pus through bronchi will cause an air-fluid level appearance.
It is characterized on CT with a thick irregular wall and inner margin, enhanced after contrast, often surrounded by consolidation causing poorly defined outer margins (Fig. 8).

Axial post-contrast CT image of the chest in the mediastinal window (A) and the lung window (B) of a 17-year-old male, showing an abscess in the middle lobe of the lung, with air–liquid content and a thick, irregular and enhanced wall
An infected necrotic neoplasm is a differential diagnosis that should be recalled especially in older patients and smokers, as it can mimic an abscess [14].
Septic emboli
Septic emboli are due to hematogenous dissemination; the infectious starting point is generally a right endocarditis, a septic thrombophlebitis, or an infected venous catheter. It is also frequently seen in cases of substance addiction.
It manifests on CT as bilateral asymmetrical alveolar nodules, that can excavate and converge. They are more predominant in the periphery and at the bases. And they often (54% of cases) have a feeding vessel. Wedge-shaped peripheral opacities are also a common manifestation (Fig. 9) [15].

Sagittal reconstruction CT image of the chest in the lung window of an 18-year-old male, showing septic emboli manifesting as multiple peripheral nodules, some of which are excavated, and some of which are triangular in shape
Hydatidosis
Hydatidosis or Echinococcosis is a parasitic infection due to Echinococcus Granulosus that occurs due to Echinococcal eggs swallowing, which often happens in rural areas, and when there is contact with contaminated dogs. It is most often asymptomatic apart from complications.
Lung is the second most common site of infection after the liver.
In the early stages of the disease, it manifests on CT as an oval or round-shaped liquid collection, except when a complication occurs:
-
In case of fissure: It can manifest as a crescentic air collection topping the cyst. Or it manifests as air bubbles within the endocyst (sometimes it translates superinfection instead of fissure) (Fig. 10).
Fig. 10 
Axial CT image of the chest in the lung window, showing a right lung hydatid cyst with air bubbles within (due to fissure)
-
In case of rupture: An image of floating membrane appears; an irregular air-fluid level with detached wall membranes giving the appearance of a “Water-lily” (Fig. 11).
Fig. 11 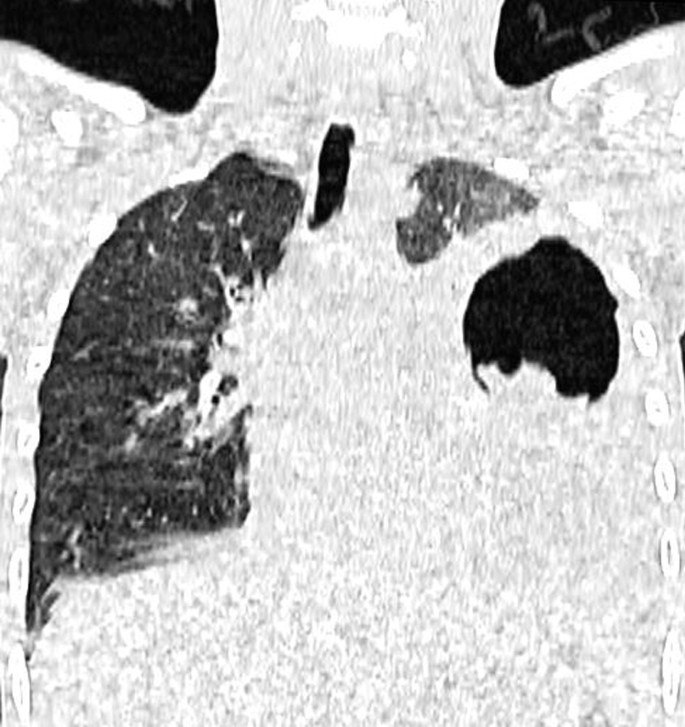
Coronal reconstruction CT image of the chest in the lung window of a 17-year-old male, showing a left lung hydatid cyst containing air, liquid, and a floating membrane giving the "water-lily" sign, (due to rupture)


Ring enhancement of the pericyst after contrast indicates infection or cyst–bronchial tree communication. The differential diagnosis of infected hydatid cysts are abscesses and neoplasms due to the high density content [16, 17].
Aspergillosis
Aspergillosis is a fungal infection, caused by inhaling spores of the aspergillus species, which is a group of saprophytic fungi.
The patient could be asymptomatic, or present with thoracic pain, hemoptysis, and fever.
We distinguish three entities that could cause cavitary lesions:
-
Aspergilloma:
It is an aspergillus colonization of a residual cavity (most commonly a tuberculosis residual cavity).
On CT it manifests as a cavity in an upper lobe or a Fowler segment, containing a well-defined oval or round mass (called fungus ball), dense, and mobile when the patient changes position. When the fungus ball is small, it makes the appearance of “Monod” sign. On the other hand, when the fungal ball almost entirely fills the cavity, only an air-crescent topping the mass is seen (Fig. 12). A CT scan of the chest can be performed in the prone position to demonstrate the mobility of the mass [6].
Fig. 12 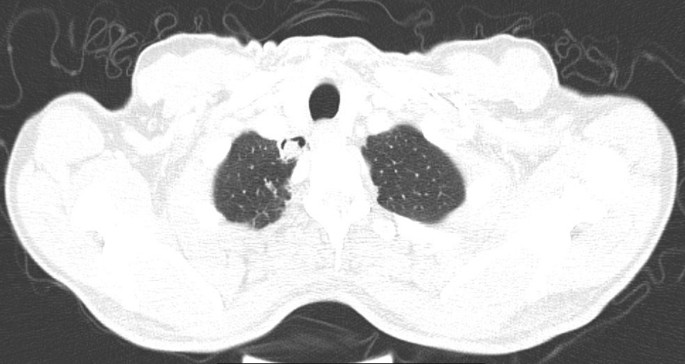
Axial CT image of the chest in the lung window of a 59-year-old male, showing an aspergilloma in the right apex of the lung, manifesting as a cavitary lesion filled with a round solid mass, topped by air in a crescentic shape
-
Subacute invasive pulmonary aspergillosis:
It develops in patients with chronic pulmonary diseases (like chronic obstructive pulmonary disease), and/or in patients with moderate immunosuppression such as diabetes, patients on corticosteroids, malnutrition, and advanced age.
On CT, it manifests as a progressive setting on weeks or months of a consolidation, usually found in an upper lobe, followed by excavation with an air-crescent sign (which reflects worsening of the disease).
The cavity can be filled with a fungus ball giving the appearance of “Monod” sign. Adjacent pleural thickening may occur [18].
-
Angio-invasive aspergillosis:
It occurs in a patient with profound immunosuppression; recent history of neutropenia, allogeneic stem cell transplantation or solid organ transplantation, prolonged use of corticosteroids or use of immunosuppressants.
It is a disseminated invasive aspergillosis, causing an occlusion of small arteries by mycelial filaments.
It manifests on CT as solitary or multiple solid nodules or masses, which could be surrounded by ground glass (due to perilesional hemorrhage). Next, excavation of the lesion occurs, presenting as an air-crescent sign that tends to appear in the recovery phase of neutropenia. The peripheral ground glass, on the other hand, tends to resolve progressively with evolution.
The reverse halo sign can also be seen, but it is a sign that is more suggestive of mucormycosis than aspergillosis [19,20,21].

Pneumocystosis
Pneumocystosis is an opportunistic fungal infection due to Pneumocystis Jirovecii.
It is typically seen in patients with a CD4 lymphocytes count below 200 cells/μl, and it is the most frequent cause of cavities in HIV patients.
On CT, it presents as areas of ground glass (or sometimes consolidation) as the most common manifestation, reflecting alveolitis. It is often isolated and can be associated with reticulations or septal thickening, and with small cysts sitting within the ground glass. The ground glass opacities have a central distribution with relative peripheral sparing in 41% of cases, a mosaic pattern in 29%, and a diffuse distribution in 24% of cases (more common in non-infected HIV patients).
An upper lobe predominance has been described.
The cysts correspond to necrosis; they are present in 10% of cases and are more frequent in HIV-infected patients than patients without HIV. They can be single or multiple, round or oval, with a thin wall, and are associated with a higher risk of pneumothorax (Fig. 13) [22, 23].

Axial CT image of the chest in the lung window of a 67-year-old male, showing central areas of ground glass and crazy paving, with cysts within, in a patient with pneumocystosis. Note an associated mild bilateral pleural effusion
Infectious pneumatocele
It is due to obstruction of a bronchiole, which causes air trapping.
Infectious pneumatoceles have been described most frequently as a complication of aerogenous staphylococcal pneumonia in children.
It manifests as a cyst with total air content or air–liquid content, it can be of any size, round or oval, and it communicates with a bronchus.
It may occur early during the infection, or late after the infection (Fig. 14) [24, 25].

Axial CT image of the chest in the lung window of a 41-year-old male, showing an area of consolidation in the right lower lobe associated with pneumatoceles in a context of staphylococcal pneumonia
Neoplastic
Primary tumors
They occur more frequently in cigarette smokers.
When patients are symptomatic, they commonly present with hemoptysis, coughing, shortness of breath, chest pain and persistent infections.
Excavation of the tumoral mass or nodule happens approximately in 2 to 16% of cases, due to central necrosis.
Epidermoid carcinoma of the lung, also known as squamous cell carcinoma, is the histological type that most often excavates [26].
It manifests on CT as a cavity that has a thick irregular wall. The content can be totally aerial (Fig. 15), or mixed; solid, liquid (necrosis and blood or infection), or both [27].

Coronal reconstruction CT image of the chest in the lung window of a 70-year-old male, showing in the left superior lobe an excavated mass with a thick wall, irregular margins and a totally air content, proven to be an epidermoid carcinoma on pathology. To note bilateral pulmonary emphysema, more marked in the right superior lobe
Association with lymphadenopathies, metastatic lung nodules, pleural effusion or pleural thickening are often seen.
Metastases
They typically appear as multiple sharp spherical nodules.
Excavation of metastases is not very frequent. It commonly happens when the primary tumor is an epidermoid carcinoma, and under chemotherapy (Fig. 16) [28, 29].

Sagittal reconstruction CT image of the chest in the lung window of a 63-year-old female, showing lung nodules, some of whom are excavated, in a patient on chemotherapy for a metastatic invasive ductal carcinoma of the breast
To note that a feeding artery can be seen in small metastases [30].
Immunologic (autoimmune)
Cavitary lesions of immunologic origin are easy to link to the disease when history of the disease is known, and when the clinical and biological contexts are suggestive.
Granulomatosis with polyangiitis
It is a necrotizing granulomatous vasculitis of small and medium-sized arteries, that affects preferentially the lungs (90%), the ENT sphere, the trachea-bronchial tree, and kidneys).On imaging nodules are commonly multiple, bilateral and scattered, commonly ranging from 2 to 4cm in size, and they excavate in more than 25% of cases, especially the nodules above 2cm, giving the appearance of a cavity with a thick wall that becomes more and more thin with evolution (Fig. 17) [31, 32].

Axial CT image of the chest in the lung window of a 56-year-old male, showing bilateral excavated nodules in a patient followed up for granulomatosis with polyangiitis
Rheumatoid arthritis
Rheumatoid nodules are not frequently seen in rheumatoid arthritis (10–22% of cases), and they reflect a good prognosis.
They tend to present as multiple nodules (≥ 4 nodules) that are peripherally located with smooth borders, and surrounded by small satellite nodules which can give the appearance of a subpleural rind of soft tissue due to coalescence. Cavitation is seen in 18% of cases (Fig. 18) [33].

Axial CT image of the chest in the lung window of a 45-year-old female, showing confluent peripheral lung nodules, enclosing air (excavation), in a patient followed-up for rheumatoid arthritis
Others
Langerhans cell histiocytosis
Langerhans cell histiocytosis is a multisystemic disease of unknown etiology, characterized with an infiltration by specialized histiocytes called Langerhans cells [34].
There is evidence of causal relationship between cigarette smoking and pulmonary Langerhans cell histiocytosis.
Lung involvement in this disease is marked by the presence of bilateral lung centrilobular nodules and micronodules, primarily concentrated in the middle and upper regions. These nodules gradually progress and develop into excavations, initially resembling thick-walled cysts that progressively become thinner, indicating an advanced stage of the disease. During this late stage, the cysts frequently merge, resulting in an irregular and distinctive shape called “bizarre shape” (Fig. 19) [35].

A schema showing the evolution of a lung nodule in Langerhans cell histiocytosis
Pulmonary infarction
Pulmonary infarction complicates pulmonary embolism, and it manifests on CT as a peripheral consolidation, triangular in shape, with a large pleural base and an apex oriented toward the hilum, containing air lucencies (air bubbles more visible in the mediastinal window), with diminished enhancement of the parenchyma involved, it gives the appearance of a reversed halo sign (Fig. 20) [36].

Axial CT angiography image of the chest in the mediastinal window of a 56-year-old male, showing a pulmonary infarction in the right lowed lobe manifesting as a consolidation, with a large pleural base, enclosing air lucencies, keeping with a pulmonary infarction. Note the arterial filling defect in the right lower pulmonary artery
Traumatic pneumatocele
Traumatic pneumatocele is due to a laceration in the lung parenchyma with retraction of the parenchyma surrounding it.
It is a round or oval cyst, single or multiple, filled with air, blood or both. It is usually surrounded by a contusion in the acute setting (Fig. 21) [37].

Axial CT image of the chest in the lung window of a 44-year-old female, showing multiple pneumatoceles in the right lower lobe, surrounded by contusion in post-trauma context. A pneumothorax, rib fractures and subcutaneous emphysema are associated
Rare etiologies
Congenital
Congenital pulmonary airway malformation
It is an abnormal bronchial proliferation during the embryonic life, with formation of communicating cysts.
Involvement is often unilateral in the lower region of the lung. They can have a purely air content, or air–liquid content.
We distinguish 5 histological types: Type 0 (lethal post-natally), type 1, 2, 3, and 4:
-
Type 1: The most common type; One or more large cysts (3–10 cm).
-
Type 2: Multiple cysts with a diameter from 0.5 to 2 cm.
-
Type 3: Microcysts (0.2 cm), that can only be seen on histologic evaluation, affecting a whole lobe or a whole lung, appearing as a homogeneous soft tissue density mass on imaging.
-
Type 4: Hamartomatous malformation involving a single lobe [38, 39].
Other studies suggested that cysts between 2.8 and 7.9 cm in size were likely to be type 1. Smaller cysts (< 2.8 cm) were more likely to be type 2, and larger cysts (> 7.9 cm) were more likely to be type 4. And that the incidence of pneumonia was higher in type 2 than in types 4 and 1. And that the frequency of mediastinal shift and pneumothorax was statistically significant, and both were more common in type 4 [40].
Bronchogenic cyst
It is a congenital malformation characterized with an intrathoracic cystic derivative of the foregut with respiratory differentiation. They can have a purely air content, or air–liquid content.
The mediastinal location is more frequent than the pulmonary location.
Intrapulmonary bronchogenic cyst on CT is generally a unilocular or multilocular mass, round, well circumscribed, located usually in the lower lobe. It can have liquid density, or high density (due to proteinaceous content), or air density (Fig. 22) [41].

Axial CT image of the chest in the lung window of a 43-year-old male, showing an intrapulmonary bronchogenic cyst in the right lower lobe
Pulmonary sequestration
Pulmonary sequestration is a territory of the lung that corresponds to a segment or a lobe which does not communicate with the tracheobronchial tree nor with the pulmonary arteries (which permits the diagnosis on CT). It is supplied by the systemic circulation, most commonly, the descending aorta.
It is often located in the left lower lobe.
We distinguish intra-lobar (ILPS) and extra-lobar pulmonary sequestration (ELPS):
-
ILPS: The most common. It presents later in childhood with recurrent infections, and its venous drainage is often towards the pulmonary veins.
-
ELPS: Is less frequent. It presents in the neonatal period with respiratory distress, and its venous drainage is toward the systemic veins into the right atrium.
ILPS can present on imaging as multiple cystic areas, cavitation, focal bronchiectasis, or areas of atelectasis. ELPS tends to appear as a well-defined solid mass [39, 42].
Others
Sarcoidosis
It is a systemic granulomatosis, affecting most commonly the lung parenchyma and/or mediastino-hilar lymph nodes. It is asymptomatic in most cases, and when it is symptomatic, cough and dyspnea are the most usual symptoms.
On CT, it often exhibits multiple micronodules and nodules with peri-lymphatic and upper lobes predominance, which can merge forming pseudo-masses of fibrosis.
It can present with mediastinal and hilar lymphadenopathies that can calcify.
Excavation in sarcoidosis is rare and usually occurs in active severe sarcoidosis. Moreover, it is often located in the middle and upper lobes, and in the hilar and posterior regions, usually seen within an alveolar consolidation and fibrotic lesions (Fig. 23) [43].

Axial CT image of the chest in the lung window of a 62-year-old female, showing bilateral perihilar alveolar infiltrate, with excavation in the left, in a patient followed up for sarcoidosis
Pneumoconiosis
Silicosis and coal workers pneumoconiosis are characterized by the presence of small nodules distributed in the upper zones of the lung, with a posterior predominance. These nodules tend to coalesce and form massive fibrotic lesions, in which cavitation can occur.
To note that mediastino-hilar lymphadenopathies are associated, with a tendency to calcify in an eggshell [44].
Lymphangioleiomyomatosis (LAM)
It is a disease that affects women at reproductive age and is characterized by a smooth muscle proliferation in the lung parenchyma, which obstructs bronchioles, and causes air entrapment and cyst-like spaces.
The pathogeny of this disease is associated with tuberous sclerosis complex mutations (TSC1 or TSC2) and estrogenic influence.
We distinguish 2 types: The sporadic LAM, and LAM with tuberous sclerosis.
It manifests on CT as multiple, bilateral, and diffuse round cysts of variable size (often small), with a thin wall (Fig. 24). Some interstitial changes such as reticulations and thickening of interlobular septa, and ground glass can also be seen.

Axial CT image of the chest in the lung window of a 29-year-old female, showing sparse small parenchymal cysts in a patient diagnosed with tuberous sclerosis keeping with LAM
It can be associated with renal angiomyolipomas or chylous effusions in tuberous sclerosis complex.
Pneumothorax is a possible complication.
The diagnosis generally requires a lung biopsy in cases where tuberous sclerosis complex is absent [45, 46].
Conclusions
Cavitary lesions have multiple etiologies; considering the epidemiological context, and the clinico-biological context is crucial to orient the diagnosis.
The number, size, distribution, wall, content, evolution and the associated lesions are all essential to analyze.
Abscesses, tumors, and aspergillomas are frequent diagnoses, along with tuberculosis and hydatidosis in epidemic areas.
Multiple small cavities and nodules peripherally located, and with feeding vessels, in a context of sepsis should recall septic emboli.
Small cysts should suggest pneumatocele in a context of trauma or infection, and congenital diseases should be recalled in children. If they are diffuse, they should suggest histiocytosis in smoking young men, and LAM in childbearing age women, and pneumocystosis when associated with ground glass in immunosuppressed patients.
Systemic diseases can only be evoked if their clinico-biological context and when associated lesions are suggestive.
The suggested diagnosis or (narrowed diagnoses) will aid the multidisciplinary team in moving forward with treatment options when indicated, and with further diagnostic tools such as a CT-guided biopsy when needed.
Availability of data and materials
The data that support the findings of this study are available on reasonable request from the corresponding author.
Abbreviations
- CT:
-
Computed tomography
- ENT:
-
Ear, nose and throat
- ILPS:
-
Intra-lobar pulmonary sequestration
- ELPS:
-
Extra-lobar pulmonary sequestration
- TSC:
-
Tuberous sclerosis complex
- LAM:
-
Lymphangioleiomyomatosis
References
Ben Romdhane MHB, Brillet P-Y, Brauner M (2015) « Syndrome cavitaire. EMC - Radiologie et imagerie médicale—cardiovasculaire—thoracique—cervicale. 10(2):1–17
Davis SD (1991) CT evaluation for pulmonary metastases in patients with extrathoracic malignancy. Radiology 180(1):1–12. https://doi.org/10.1148/radiology.180.1.2052672
Parkar AP, Kandiah P (2016) Differential diagnosis of cavitary lung lesions. J Belg Soc Radiol 100(1):100
Woodring J, Fried A, Chuang V (1980) Solitary cavities of the lung: diagnostic implications of cavity wall thickness. Am J Roentgenol 135(6):1269–1271
Ryu JH, Swensen SJ (2003) Cystic and cavitary lung diseases: focal and diffuse. Mayo Clin Proc 78(6):744–752
Sharma S, Dubey SK, Kumar N et al (2013) “Monod” and “air crescent” sign in aspergilloma. BMJ Case Rep. https://doi.org/10.1136/bcr-2013-200936
Cosgrove GP, Frankel SK, Brown KK (2007) Challenges in pulmonary fibrosis · 3: Cystic lung disease. Thorax 62(9):820–829
Milliron B, Henry TS, Veeraraghavan S et al (2015) Bronchiectasis: mechanisms and imaging clues of associated common and uncommon diseases. Radiographics 35(4):1011–1030
Hansell DM, Bankier AA, MacMahon H et al (2008) Fleischner society: glossary of terms for thoracic imaging. Radiology 246(3):697–722
Eren S, Çiriş F (2005) Diaphragmatic hernia: diagnostic approaches with review of the literature. Eur J Radiol 54(3):448–459
Kaur R, Prabhakar A, Kochhar S et al (2015) Blunt traumatic diaphragmatic hernia: pictorial review of CT signs. Indian J Radiol Imaging 25(03):226–232
Kraus GJ (2007) The split pleura sign. Radiology 243(1):297–298
Nachiappan AC, Rahbar K, Shi X et al (2017) Pulmonary tuberculosis: role of radiology in diagnosis and management. Radiographics 37(1):52–72
Kuhajda I, Zarogoulidis K, Tsirgogianni K et al (2015) Lung abscess-etiology, diagnostic and treatment options. Ann Transl Med 3(13):183
Owji S, Choi WJ, Al-Jabbari E et al (2022) Computed tomography findings in septic pulmonary embolism: a case report and literature review. Radiol Case Rep 17(8):2639–2642
Emlik D, Ödev K, Poyraz N et al (2015) Radiological Characteristics of Pulmonary Hydatid Cysts. In: Rodriguez-Morales AJ, éditeur. Current Topics in Echinococcosis [Internet]. InTech [cité 5 févr 2023]. Disponible sur: http://www.intechopen.com/books/current-topics-in-echinococcosis/radiological-characteristics-of-pulmonary-hydatid-cysts
Durhan G, Tan AA, Düzgün SA (2020) Radiological manifestations of thoracic hydatid cysts: pulmonary and extrapulmonary findings. Insights Imaging 11(1):116
Denning DW, Cadranel J, Beigelman-Aubry C et al (2016) Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. Eur Respir J 47(1):45–68
De Pauw B, Walsh TJ, Donnelly JP et al (2008) Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 46(12):1813–1821
Fan K, Lee C (2019) Imaging evolution of an invasive fungal infection in a neutropenic patient. Ann Am Thorac Soc 16(2):271–274
Jung J, Kim MY, Lee HJ et al (2015) Comparison of computed tomographic findings in pulmonary mucormycosis and invasive pulmonary aspergillosis. Clin Microbiol Infect 21(7):684.e11-684.e18
Kanne JP, Yandow DR, Meyer CA (2012) Pneumocystis jiroveci pneumonia: high-resolution CT findings in patients with and without HIV infection. Am J Roentgenol 198(6):W555–W561
Hidalgo A, Falcó V, Mauleón S et al (2003) Accuracy of high-resolution CT in distinguishing between pneumocystis carinii pneumonia and non-Pneumocystis carinii pneumonia in AIDS patients. Eur Radiol 13(5):1179–1184
Quigley M, Fraser R (1988) Pulmonary pneumatocele: pathology and pathogenesis. Am J Roentgenol 150(6):1275–1277
McGarry T, Giosa R, Rohman M (1987) Pneumatocele formation in adult pneumonia. Chest 92(4):717–720
Vourtsi A, Gouliamos A, Moulopoulos L et al (2001) CT appearance of solitary and multiple cystic and cavitary lung lesions. Eur Radiol 11(4):612–622
Panunzio A, Sartori P (2020) Lung cancer and radiological imaging. Curr Radiopharm 13(3):238–242
Chaudhuri MR (1970) Cavitary pulmonary metastases. Thorax 25(3):375–381. https://doi.org/10.1136/thx.25.3.375
Seo JB, Im JG, Goo JM (2001) Atypical pulmonary metastases: spectrum of radiologic findings. Radiographics 21(2):403–417
Murata K, Takahashi M, Mori M et al (1992) Pulmonary metastatic nodules: CT-pathologic correlation. Radiology 182(2):331–335
Allen SD, Harvey CJ (2007) Imaging of Wegener’s granulomatosis. Br J Radiol 80(957):757–765
Li J, Li C, Li J (2018) Thoracic manifestation of Wegener’s granulomatosis: computed tomography findings and analysis of misdiagnosis. Exp Ther Med. https://doi.org/10.3892/etm.2018.6154
Koslow M, Young JR, Yi ES et al (2019) Rheumatoid pulmonary nodules: clinical and imaging features compared with malignancy. Eur Radiol 29(4):1684–1692
Grana N (2014) Langerhans cell histiocytosis. Cancer Control 21(4):328–334. https://doi.org/10.1177/107327481402100409
Suri HS, Yi ES, Nowakowski GS et al (2012) Pulmonary langerhans cell histiocytosis. Orphanet J Rare Dis 19(7):16. https://doi.org/10.1186/1750-1172-7-16
Naggar A, Benmoussa M, El Fenni J (2023) The most typical appearance of pulmonary infarction on computed tomography. Visual J Emerg Med 31:101698
Kaewlai R, Avery LL, Asrani AV et al (2008) Multidetector CT of blunt thoracic trauma. Radiographics 28(6):1555–1570
Bolde S (2015) Congenital pulmonary airway malformation: a report of two cases. World J Clin Cases 3(5):470
Odev K, Guler İ, Altinok T et al (2013) Cystic and cavitary lung lesions in children: radiologic findings with pathologic correlation. J Clin Imaging Sci 3:60
D’Hondt D, Van Hoyweghen A, Broeckx G et al (2021) An incidental finding of congenital pulmonary airway malformation type 3 during a forensic autopsy for a sudden infant death: a case report with a brief literature review. Am J Forensic Med Pathol 42(3):301
Suen HC, Mathisen DJ, Grillo HC et al (1993) Surgical management and radiological characteristics of bronchogenic cysts. Ann Thorac Surg 55(2):476–481
Corbett HJ, Humphrey GME (2004) Pulmonary sequestration. Paediatr Respir Rev 5(1):59–68
Hours S, Nunes H, Kambouchner M et al (2008) Pulmonary cavitary sarcoidosis: clinico-radiologic characteristics and natural history of a rare form of sarcoidosis. Medicine 87(3):142–151
Akira M (2002) High-resolution CT in the evaluation of occupational and environmental disease. Radiol Clin North Am 40(1):43–59
Sherrier R, Chiles C, Roggli V (1989) Pulmonary lymphangioleiomyomatosis: CT findings. Am J Roentgenol 153(5):937–940
McCormack FX (2008) Lymphangioleiomyomatosis. Chest 133(2):507–516
Acknowledgements
Not applicable.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
All authors contributed significantly to the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Naggar, A., Laasri, K., Berrada, K. et al. Differential diagnoses of cavitary lung lesions on computed tomography: a pictorial essay. Egypt J Radiol Nucl Med 54, 149 (2023). https://doi.org/10.1186/s43055-023-01098-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-01098-7