- Research
- Open access
- Published:
Role of conventional ultrasound and shear wave elastography of median nerve in diagnosis and differentiation of carpal tunnel syndrome severity in correlation with electrodiagnostic studies
Egyptian Journal of Radiology and Nuclear Medicine volume 55, Article number: 53 (2024)
Abstract
Background
The gold standard for CTS diagnosis is abnormalities on electrophysiologic testing in conjunction with specified symptoms. Electrophysiologic testing can also identify the severity of nerve injury.
Aim of work
Aimed to investigate how effective various ultrasonography and elastography parameters at diagnosing and grading the severity of carpal tunnel syndrome in correlation with the electrophysiological evaluation of the median nerve.
Methods
The study included 62 wrists, 31 CTS cases and 25 females. Thirty-one healthy adults served as control group. Eleven males (35.5%) and 20 females (64.5%) were included. All US examinations were done with the subjects sitting with their upper limbs relaxed on a pillow with forearm in supine position, and the fingers are semi-flexed. Ultrasound and elastography parameters were recorded. NCS was done by recording median nerve motor and sensory functions and then comparing median nerve versus radial and ulnar nerves if the previous recordings were normal to detect early starting cases.
Results
US and elastography can significantly diagnose CTS and detecting its severity (mild/moderate versus severe CTS).
Conclusions
It is noninvasive to examine the median nerve using ultrasound and shear wave elastography, highly sensitive diagnostic modality. It can significantly diagnose CTS and severity of CTS (in contrast to mild, moderate, and severe instances). Mixing high-resolution conventional B-mode US with shear wave ultrasound elastography of the median nerve may increase the diagnostic precision of CTS.
Background
Compression neuropathies are common, with carpal tunnel syndrome (CTS) being the most common kind. It usually manifests between the ages of 45 and 60, and it strikes females more than males. Patients usually describe symptoms like “my hands fall asleep” or “things slip out of my fingers without me even realizing it.” Typical symptoms include numbness and tingling in the first three fingers and the radial half of the fourth digit. Some patients have symptoms only at specific times, whereas others are awakened from sleep [1].
The gold standard for CTS diagnosis is abnormalities on electrophysiologic testing in conjunction with specified symptoms. Electrophysiologic testing can also identify the severity of nerve injury. CTS is typically classified as mild, moderate, or severe. On electrophysiologic testing, mild CTS patients exhibit sensory abnormalities alone, while moderate and severe CTS patients have sensory and motor abnormalities [2].
Improvements in technology and software have made high-resolution ultrasonography a powerful tool for visualizing peripheral nerves. As a result, it has been included in the standard diagnostic process for people who have carpal tunnel syndrome. Understanding the normal sonographic appearances of the median nerve/carpal tunnel, as well as the direct pathophysiological manifestations of compressing neuropathy based on the median nerve’s sonographic appearance, helps diagnose carpal tunnel syndrome using sonography [1].
Sonoelastography is a straightforward noninvasive imaging method. The use of sonoelastography for the assessment of neuromuscular diseases has recently gained popularity. Sonoelastography is a technique that uses ultrasound to assess and measure soft tissue stiffness [3].
Imaging of tiny musculoskeletal structures, including the peripheral nerve, are possible with high-resolution ultrasonography. When compared to electrophysiological testing and other imaging techniques like MRI [1], it is more accessible, less expensive, and less intrusive.
The purpose of this study was to compare the electrophysiological assessment of the median nerve to the results of different ultrasonography and elastography parameters for the diagnosis and severity grading of carpal tunnel syndrome.
Methods
The reviewing board and the ethics committee at Cairo University’s School of Medicine have both given their clearance to this work. Sixty-two wrists were used in the investigation. From December 2021 to June 2022, the neurophysiology department at Cairo University Hospitals sent 31 wrists of CTS patients to the radiology department for further imaging and diagnostic testing. The control group consisted of 31 adult wrists that had no abnormalities. The included cases have been clarified about the aim and the procedure of this study, and verbal consent has been taken from the cases before the study.
Inclusion criteria
Patients suspected clinically by CTS (swelling, pain, paraesthesia, numbness or weakness of the hand, sensory deficit or atrophy of the thenar muscles) and confirmed as CTS by electrodiagnostic studies.
Exclusion criteria
Recent carpal tunnel-releasing surgery or previous wrist or hand fractures and neuropathies due to diabetes mellitus, hyperthyroidism, and polyneuropathy.
Radiological examination
The machine used is a Toshiba Aplio 500 with a linear probe of 7–14 MHz frequency, and images were interpreted by a musculoskeletal U/S consultant with an experience of 10 years.
Patient positioning
All patients were asked to sit facing the examiner with relaxed upper limbs on a pillow and the forearm in a supine position; the fingers were allowed to hang loosely while in a semi-flexed posture. During the whole sonographic test, patients were asked to keep their wrists and fingers completely still. Exams were performed with the patient’s arms and hands at rest to prevent aggravating carpal tunnel syndrome.
The following data were recorded: The demographics of the participants including age, sex, and laterality of the examined hand (right or left). The electrophysiological diagnosis states the degree of severity of CTS (mild, moderate, or severe). Median nerve cross-sectional area at the wrist level using the scaphoid and pisiform bones as reference points, the carpal tunnel entrance was evaluated for median nerve CSA. Delta cross-sectional area by subtracting the CSA of the median nerve at the surface of the pronator quadrates muscle from the CSA of the nerve at the entrance to the carpal tunnel, we were able to calculate the median nerve’s delta cross-sectional area. By comparing the median nerve’s CSA at the level of the carpal tunnel entrance to its CSA 12 cm proximal to the distal wrist crease, a wrist-forearm ratio may be determined. Shear wave elastography on sagittal ultrasound pictures and proximal carpal row elastography measures were taken. At the level of the lunate bone, a region of interest (ROI) was established, including the median nerve. Care was taken to avoid the compression effect of the transducer; this was achieved by applying copious amounts of gel. Vascularity color Doppler was applied to the nerve to detect the presence of vascularity.
Electrodiagnostic studies
The Nihon Kohden Neuropak MEB-9200G/K EP/EMG measurement system, version 08.1, Japan, was used for the electrophysiological studies. The examination was performed and interpreted by a neurophysiologist having experience of 13 years.
The following tests were performed:
Median motor conduction studies
Recorded from the abductor pollicis brevis muscle (to obtain distal motor latency, amplitude, and conduction velocity).
Median sensory studies
Recorded from the index finger (to obtain peak sensory latency and amplitude). Comparative studies median vs. radial (thumb) and median vs. ulnar (4th digit) if the previous studies were normal to detect early starting cases.
Ethical approval
Patients were provided comprehensive trial information, and the research was authorized by the Cairo University Ethics Board. Everyone who took part in the study gave their informed consent in writing. All research involving human participants in this study followed the guidelines established by the World Medical Association in their 1975 Declaration of Helsinki.
Statistical analysis
It was done using SPSS 22; the chi2 test was used to compare categorical data reported as frequencies and percentages. When comparing more than two groups, we used the student T test for means and the one-way analysis of variance for continuous variables. Sensitivity and specificity analyses were performed to determine the diagnostic threshold for CTS and for severe CTS. The cutoff for significance was set at a p-value of 0.05.
Results
The participants of this study included 62 wrists; 31 wrists were diagnosed as carpal tunnel syndrome through electrophysiology assessment of the median nerve and 31 normal wrists were regarded as controls (they are healthy volunteers not complaining of any symptoms) as shown in Table 1.
The electrophysiological study assessment of the cases group was performed as a gold standard exam to classify the cases; the cases were classified as mild, moderate, and severe according to the Padua classification scale [4]. Just short of half of the included wrists of the cases group were found to have a moderate degree of carpal tunnel syndrome; those wrists with the most severe type of carpal tunnel syndrome accounted for less than 20% of all cases. About a third of the affected wrists had just mild carpal tunnel as shown in Table 2, Fig. 1.

Bar chart showing electrophysiological grade of the examined wrists with CTS
The neurophysiological and radiological studies were performed at the same day or with maximum 4 days apart.
-
Radiological exam: Vascularity of median nerve was reported in 26% of the included individuals; comparison between study groups showed that 51% in cases groups had nerve vascularity, while 0% had it in control group with p value 0.0001 as shown in Tables 3, 4.
Table 3 Description of ultrasound and elastography findings among cases and control groups Table 4 Vascularity of median nerve detected in CTS different sub-groups
Diagnosis of CTS
Median nerve CSA can significantly predict carpal tunnel syndrome with a p-value of 0.001 using a cutoff of 9.8 mm, sensitivity 87.1%, specificity 83.9%, and AUC 89.9%.
Delta CSA can significantly predict carpal tunnel syndrome with a p-value of 0.001 using a cutoff of 2.6 mm, sensitivity of 90.3%, specificity of 83.9%, and AUC of 94.2%.
The wrist/forearm ratio of median nerve CSA can significantly predict carpal tunnel syndrome with a p-value of 0.001 using a cutoff of 1.35 mm, sensitivity of 93.5%, specificity of 71%, and AUC of 88.8%.
Shear wave at the wrist can significantly predict carpal tunnel syndrome with p value of 0.001 using a cutoff of 51 Kpa, sensitivity of 100%, specificity of 96.8%, and AUC of 99.8% as shown in Fig. 2.

ROC curve showing predictability of ultrasound for carpal tunnel syndrome
Diagnosis of severe CTS
Median nerve CSA can significantly predict severe carpal tunnel syndrome with a p-value of 0.003 using a cutoff of 14.5 mm, sensitivity of 100%, specificity of 84.6%, and AUC of 92.7%.
Delta CSA can significantly predict severe carpal tunnel syndrome with a p-value of 0.003 using a cutoff of 8 mm, sensitivity of 100%, specificity of 80.8%, and AUC of 93.1%. Wrist/forearm ratio nerve can significantly predict severe carpal tunnel syndrome with a p-value of 0.001 using a cutoff of 2.4 mm, sensitivity of 100%, specificity of 96.2%, and AUC of 98.1%. Shear wave at the wrist can significantly predict severe carpal tunnel syndrome with p-value of 0.001 respectively using a cutoff of 106.2 Kpa, sensitivity of 100%, specificity 96.2%, and AUC 99.2% as shown in Table 5, Fig. 3

ROC curve showing predictability of ultrasound for severe carpal tunnel syndrome
Comparing individuals with mild or moderate carpal tunnel condition to those in severe disease using sub-group analysis of the cases group, we found that the postulated ultrasonography and elastography parameters were significantly greater among people with severe disease (p 0.001, p 0.001, p 0.001, and p = 0, respectively) than those with mild or moderate disease as shown in Table 5
-
Correlation between ultrasound and elastography parameters and electrophysiological grade of carpal tunnel severity:
Sub-group analysis of the cases group was done to correlate the electrophysiological degree of carpal tunnel syndrome severity to the postulated ultrasonography and elastography parameters investigated in our study, and comparison of mean median nerve CSA, delta CSA, wrist/forearm ratio and shear wave elastography is significantly higher among patients with severe carpal tunnel syndrome compared to those with mild or moderate disease with p values 0.001, 0.001, 0.001 and 0.001, respectively (Table 6; Figs. 4, 5, 6 and 7).
Table 6 Correlation between the study parameters and grade of CTS Fig. 4 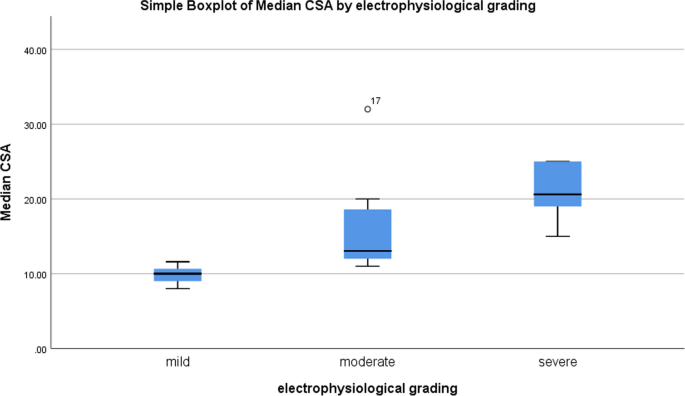
Box plot showing correlation between electrophysiological grade and median nerve CSA
Fig. 5 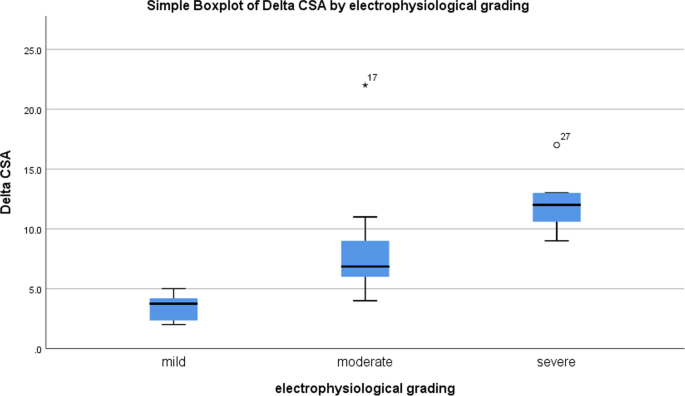
Box plot showing correlation between electrophysiological grade and delta CSA
Fig. 6 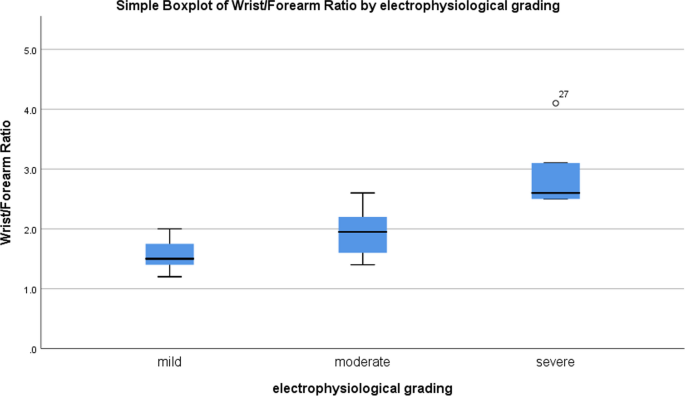
Box plot showing correlation between electrophysiological grade and wrist\forearm ratio
Fig. 7 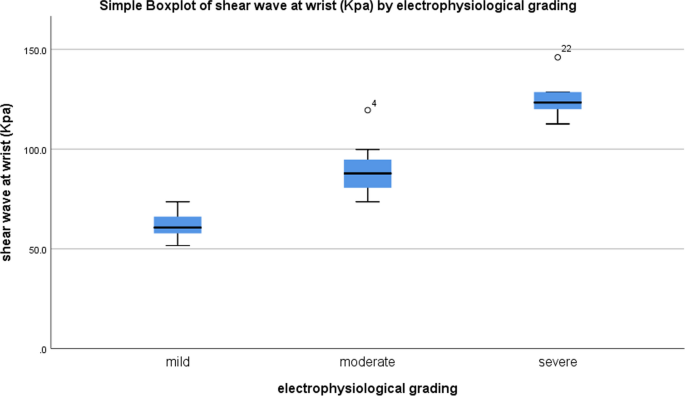
Box plot showing correlation between electrophysiological grade and shear wave at wrist (Kpa)




Case presentation
-
I.
A 30-year-old female control case with no complaints (Fig. 8a, b, c).
Fig. 8 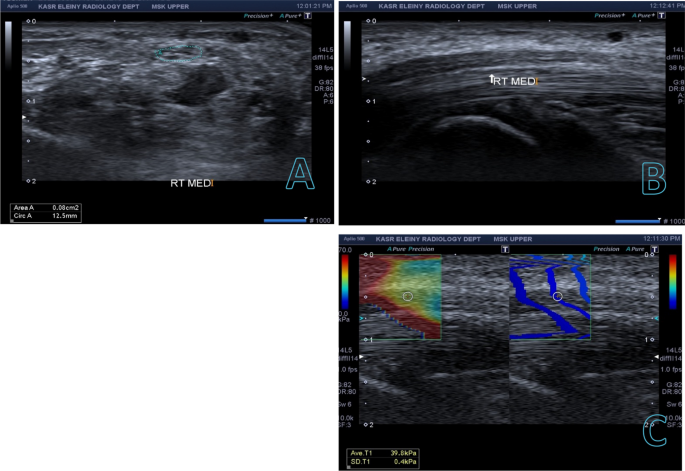
a B-mode assessment of the right median nerve in TS revealed within normal cross-sectional area measuring 0.08 cm2 b B-mode image shows the longitudinal axis of the right median nerve with normal echogenicity c The picture on the right is the B-mode, while the image on the left assesses the median nerve’s elasticity using a color-coded box, circular ROI for quantitative measurements, and a color code scale at the top of the image. The SWE reading was 39.8 kPa
-
II.
A 47-year-old female patient came complaining of pain, tingling and paresthesia involving right lateral three and half fingers. NCS revealed mild entrapment of the right median nerve at the level of the wrist (Fig. 9a, b, c).
Fig. 9 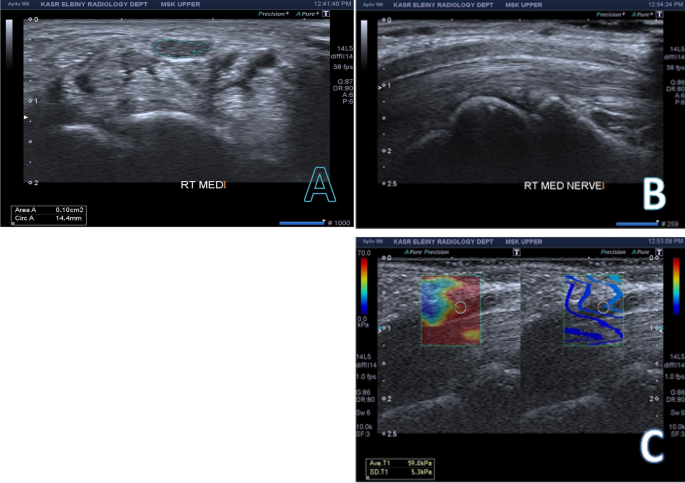
a B-mode assessment of median nerve revealed cross-sectional area of 0.10 cm2. b B-mode image shows the longitudinal axis of the RT median nerve c An image measuring the elasticity of the median nerve (59.8 kPa) with a color-coded box, circular ROI for quantitative measurements, and a color code scale at the top side of the image
-
III.
A 24-year-old female patient came complaining of pain and paresthesia involving left lateral three and half fingers referred to her forearm. NCS revealed mild entrapment of the left median nerve at the level of the wrist (Fig. 10a, b, c).
Fig. 10 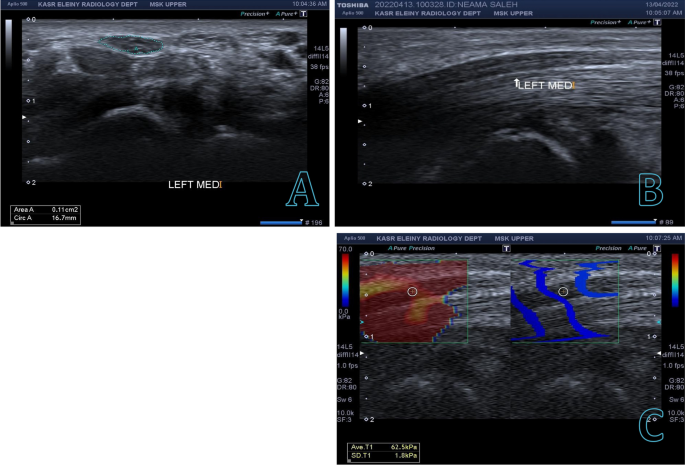
a B-mode assessment of median nerve revealed cross-sectional area of 0.11 cm2 b B-mode image shows the longitudinal axis of the left median nerve. c The right image is the B-mode, the left image measures the elasticity of the median nerve (62.5 kPa) with a color-coded box, circular ROI for quantitative measurements and a color code scale at the top side of image
-
IV.
A 35-year-old female patient came complaining of pain and paresthesia involving right lateral three and half fingers with sudden fall of objects out of her hands. NCS revealed: Severe entrapment of the right median nerve at the level of the wrist (Fig. 11a, b, c).
Fig. 11 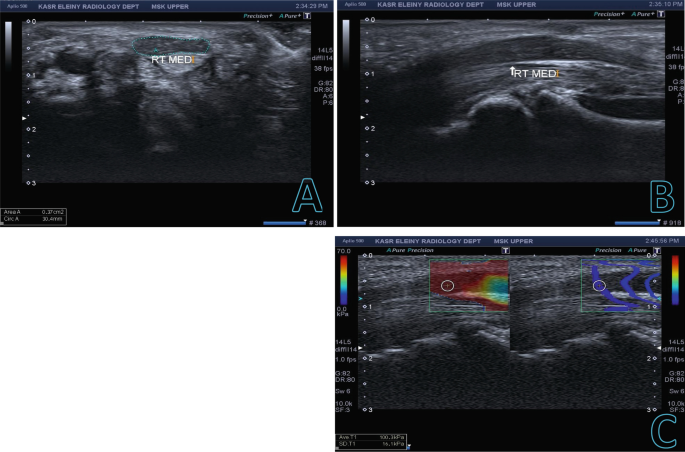
a B-mode assessment of median nerve revealed cross-sectional area of 0.37 cm2. b B-mode image shows the longitudinal axis of the right median nerve, showing decreased nerve echogenicity and abrupt change in the nerve caliber. c Image measures the elasticity of the median nerve (100.3 kPa) with a color-coded box, circular ROI for quantitative measurements and a color code scale at the top side of image
-
V.
A 56-year-old female patient came complaining of persistent paresthesia involving right lateral three and half fingers which is more severe at night. NCS revealed: Severe entrapment of the right median nerve at the level of the wrist (Fig. 12a, b, c).
Fig. 12 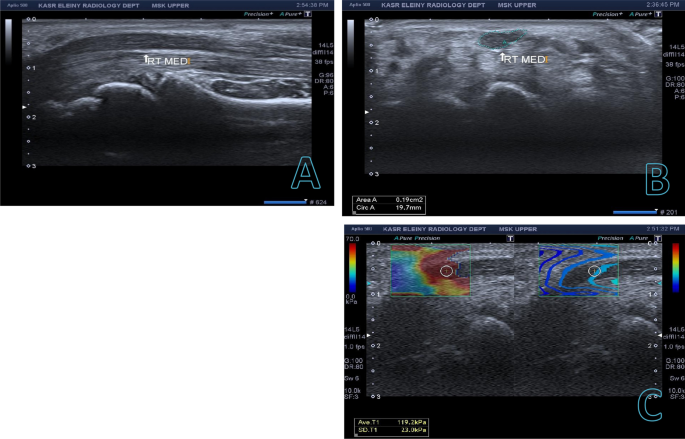
a B-mode assessment of median nerve revealed cross-sectional area of 0.19 cm2. b B-mode image shows the longitudinal axis of the right median nerve, showing decreased nerve echogenicity c The right image is the B-mode, the left image measures the elasticity of the median nerve (119.2 kPa) with a color-coded box, circular ROI for quantitative measurements and a color code scale at the top side of image





Discussion
The study aimed to investigate the accuracy with which various ultrasonography and elastography characteristics diagnose and grade carpal tunnel syndrome.
This study included 62 wrists; 31 wrists were diagnosed as carpal tunnel syndrome through electrophysiology assessment of median nerve and 31 normal wrists were regarded as controls. 27.4% of the participants were males, while 72.6% were females.
We evaluated the median nerve using imaging techniques such as cross-sectional area (CSA), delta CSA, wrist-to-forearm ratio, shear wave elastography, and vascularity. The sensitivity and specificity of each of the first four criteria was measured to evaluate their diagnostic effectiveness in distinguishing cases from controls. The threshold value for each variable was calculated.
After looking into the median nerve CSA, we discovered that the patients had a mean value of 14.04 mm2, while the controls had a mean value of 8.32 mm2. With a P value of 0.0001, a mean value of 9.83 mm2 is indicative of mild CTS, whereas values of 15.21 mm2 and 20.92 mm2 are indicative of moderate and severe CTS, respectively. The diagnostic performance for CTS improved to 87.1% at a cutoff value of 9.8 mm2, with a specificity of 83.9%.
Our findings are consistent with a case control study which reported that ultrasound can significantly diagnose CTS using median CSA with a cutoff point 8.5 mm2 with sensitivity 81% and specificity 83%. This study also revealed mean CSA for cases 11.7 mm2 versus 7.2 mm2 for control with p value 0.01 [3].
The mean CSA for the patients was 11.81 mm2 and the mean CSA for the controls was 7.76 mm2; this is a statistically significant difference with p value < 0.05 which is to some extent close to our results. The authors demonstrated the limited ability of CSA in their study at grading the severity of CTS.
The 8.5 mm2 threshold was proposed for the diagnosis of CTS by Wee and Simon [5]. In contrast to our findings, which demonstrated that shear wave elastography was superior to CSA in diagnosing CTS, they have found that CSA was better than shear wave elastography in this regard. They hypothesized that since elderly CTS patients often had a lower CSA, CSA may be a less sensitive predictor for CTS in patients aged 70 and over.
Our results were in agreement with those of a case–control research by Azami et al. [6], who found that a cutoff value of 9.15 mm2 provided the highest diagnostic accuracy (99.2% sensitivity and 88.3% specificity). Median nerve cross-sectional area (CSA) was significantly larger in CTS sick hands, at 13.31 mm2, than in healthy hands, at 8.57 mm2, with a P value of 0.001. Consistent with our findings, there was a statistically significant variation in median nerve cross-sectional area between mild, moderate, and severe CTS.
The median nerve’s mean cross-sectional area was 14.9% larger in those with CTS than in people without the condition, according to another case control research. The cutoff threshold for the diagnostic of CTS was 10.5 mm2 with sensitivity 89% and specificity 94% [7].
The modest discrepancy in findings across research may be attributable to the various study designs and assessment methods used.
In this research, the ratio of the sizing of the patient’s wrist to their forearm was substantially greater in the case group (mean 1.95) than in the control group (1.26). The mean was 1.57, which is indicative of mild CTS, 1.93, which is indicative of moderate CTS, and 2.96, which is indicative of severe CTS (P 0.0001). There was a 93.5% sensitivity, a 71% specificity, and an AUC of 0.888 when using a cutoff value of 1.35 to distinguish between cases and controls.
The findings were consistent with the case control study carried by Ibrahim [3], who stated a cutoff value of 1.3 for diagnosing CTS with sensitivity 89% and specificity 87%. Similarly, Wee and Simon [5] stated that the wrist-to-forearm median nerve ratio was greater in patients with CTS compared to controls (mean 2.17 vs. 1.31 P < 0.001). They suggested a cutoff value of 1.45.
A case control study showed that the wrist/forearm ratio of median nerve CSA in healthy controls was 1.0 ± 0.1 versus 2.1 ± 0.5 among cases, using a cutoff 1.4 with sensitivity 100% and was more sensitive compared to median nerve CSA with sensitivity 93% [8].
The present investigation found that a delta CSA cutoff of 2.65 mm2 distinguished between cases and controls with a sensitivity of 90.3%, specificity of 83.9%, AUC of 0.942, and a P value of 0.001. In our investigation, the mean measurement delta CSA for the cases group was 7.03 mm2, whereas it was just 2 mm2 for the controls. With a P value of 0.0001, a mean value of 3.47 mm2 is consistent with mild CTS, 8.21 mm2 with moderate CTS, and 12.32 mm2 with severe CTS.
This finding corroborated the results of a case–control research by Klauser et al. [9], which compared 100 CTS wrists to 93 control wrists and found that the delta CSA was more useful for diagnosis than the CSA at the wrist (P = 0.036). CTS could be diagnosed with 99% sensitivity and 100% specificity when the threshold was set at 2 mm2. According to their data, the average delta CSA in symptom-free wrists was 0.25 mm2, but it was 7.4 mm2 in CTS-affected wrists (P. 01).
Our research showed an association between electrophysiological diagnostic examinations showing a higher severity grade of CTS and higher mean median nerve stiffness. Comparing median nerve shear wave analysis in cases (mean 51.6 Kpa) and controls (mean 19.9 Kpa), there was a statistically significant difference between the two groups, with the means for mild, moderate, and severe grades coming in at 61.96 Kpa, 89.02 Kpa, and 126 Kpa, respectively. Shear wave elastography was shown to be the most accurate parameter in the diagnosis of CTS when using a cutoff value of 51 kPa (sensitivity = 100%, specificity = 96.8%, and AUC = 0.998).
Our findings are consistent with a case control study which reported that ultrasound can significantly diagnose CTS through evaluating nerve stiffness by SWE using a cutoff 65.4 kPa, with sensitivity 94.6% and specificity 97.3% [3].
Our results are also consistent with those of Paluch et al. [10], who examined 87 patients and 34 controls and established a median nerve stiffness cutoff value of 79 kPa with 96.6% sensitivity and 100% specificity. The new study’s threshold and diagnosis accuracy were also quite close to these previous results.
The sensitivity and specificity of Wee and Simon [5]’s investigation of 47 wrists with carpal tunnel syndrome were 63% and 64%, respectively, making their cutoff value higher than that previously reported. They also noted a statistically significant variation in SWE among instances with varying degrees of CTS, with the mean SWE being 117.7 ± 79.3 kpa for mild cases, 144.0 ± 71.1 kpa for intermediate cases, and 196.6 ± 48.4 kpa for severe cases (p 0.0001). The author attributed the noticeable disparity in findings to the older age of the patients who participated in the research.
Our data showed that vascularity of median nerve was reported in 51% of cases groups versus 0% in control group with p value 0.0001. One of the included mild cases, ten of the included moderate cases and all the included severe cases showed vascularity.
We agreed to large extent with results reported by Ghasemi-Esfe et al. [11], concluding that nerve vascularity was reported in 100% of moderate and severe CTS cases and 91.4% in mild cases and were significantly more frequent among cases compared to control group with p value < 0.01.
Our results are consistent with Ibrahim [3], who revealed that none of controls showed positive power Doppler signals, but it was seen in 16 wrists out of 40 wrists with CTS (P = 0.001).
Another study evaluated the vascularity of median nerve and the results. In the present study, sensitivity analysis showed that median nerve CSA, delta CSA, wrist/forearm ratio and shear wave elastography at wrist can significantly predict severe carpal tunnel syndrome, using a cutoff 14.5 mm2, 8 mm2, 2.4 and 106 Kpa, respectively, with sensitivities 100% each and specificity 84.6%, 80.8%, 96.2% and 96.2%, respectively.
Our findings are consistent with the study conducted by Ibrahim [3], who reported that ultrasound can significantly determine the severity of CTS using median nerve CSA, wrist/forearm ratio with a cutoff point 16.2 mm and 3.5, with sensitivity 46%, 45% and specificity 43%, 42%, respectively, as well, nerve stiffness by SWE can significantly diagnose CTS using a cutoff 95.8 kPa, with sensitivity 96.7% and specificity 97.8%.
Emara et al. [12] suggested a cutoff value 12 mm2 for CSA to differentiate mild and moderate from severe CTS with sensitivity 85.71% and specificity 70.89%.
Comparing patients with mild and moderate carpal tunnel syndrome to those with severe disease, we found that the mean median nerve CSA, delta CSA, wrist/forearm ratio, and shear wave elastography were all significantly higher in the severe group (p 0.001, 0.001, 0.001, and 0.001, respectively).
Based on these findings, SWE showed the highest sensitivity and specificity in diagnosis of CTS compared to other parameters, as well, discrimination between mild/moderate CTS versus severe CTS. We suggest cutoff value of 51 kPa for the diagnosis of CTS. When using electrophysiology as the gold standard this value produced 100% sensitivity and 96.8%specificity.
Following SWE, delta cross-sectional areas, followed by median nerve cross-sectional area and lastly wrist-to-forearm ration.
Ultrasound and elastography measures showed a strong ability to classify patients into mild, moderate, and severe categories. It was not possible to determine cutoff values for the studied parameters that reliably distinguish between mild, moderate, and severe illness. This may be because each sub-group is rather tiny.
While we did find several limitations to this research, the most significant of these was the fact that ultrasonography is an operator-dependent technique and, as such, needs training to prevent inaccurate interpretation.
Conclusions
In summary, we found that CTS may be diagnosed using US and elastography and that diagnostic accuracy can be increased by combining several US and elastography characteristics. Sonoelastography can also be used for grading mild and moderate versus severe CTS; however, cutoff points between different sub-groups (mild, moderate, and severe) need a larger sample size.
Availability of data and material
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- CSA:
-
Cross-sectional area
- CTS:
-
Carpal tunnel syndrome
- ROI:
-
Region of interest
- SWE:
-
Shear wave elastography
References
Peer S, Gruber H, Loizides A (2012) Sonography of carpal tunnel syndrome: why, when and how. Imaging Med 4(3):287
Duncan S, Bhate O, Mustaly H (2017) Pathophysiology of carpal tunnel syndrome. In: Carpal tunnel syndrome related median neuropathies, pp 13–29
Ibrahim H (2021) Diagnostic value of median nerve shear wave ultrasound elastography in diagnosis and differentiation of carpal tunnel syndrome severity. Egypt J Radiol Nucl Med 52(1):1–10
Pauda L, Lo Monaco M, Gregori B, Valente EM, Padua R, Tonali P (1997) Neurophysiological classification and sensitivity in 500 carpal tunnel syndrome hands. Acta Neurol Scand 96(4):211–217
Wee T, Simon N (2020) Shearwave elastography in the differentiation of carpal tunnel syndrome severity. PM&R 12:1134–1139
Azami A, Maleki N, Anari H et al (2014) The diagnostic value of ultrasound compared with nerve conduction velocity in carpal tunnel syndrome. Int J Rheum Dis 17(6):612–620
Yesildag A, Kutluhan S, Sengul N et al (2004) The role of ultrasonographic measurements of the median nerve in the diagnosis of carpal tunnel syndrome. Clin Radiol 59(10):910–915
Hobson-Webb L, Massey J, Juel V et al (2008) The ultrasonographic wrist-to-forearm median nerve area ratio in carpal tunnel syndrome. Clin Neurophysiol 119(6):1353–1357
Klauser A, Halpern E, Zordo DE et al (2009) Carpal tunnel syndrome assessment with US: value of additional cross-sectional area measurements of the median nerve in patients versus healthy volunteers. Radiology 250:171–177
Paluch Ł, Pietruski P, Walecki J et al (2018) Wrist to forearm ratio as a median nerve shear wave elastography test in carpal tunnel syndrome diagnosis. J Plast Reconstr Aesthet Surg 71(8):1146–1152
Ghasemi-Esfe A, Khalilzadeh O, Mazloumi M et al (2011) Combination of high-resolution and color Doppler ultrasound in diagnosis of carpal tunnel syndrome. Acta Radiol 52(2):191–197
Emara D, ElShafey M, Naby H (2017) Ultrasound elastography in carpal tunnel syndrome (CTS): our experience in 100 patients. European Congress of Radiology-ECR 2017
Acknowledgements
Not applicable.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
IE analyzed and interpreted the results of the ultrasound and elastography studies done for the patients. AT performed and interpreted the results of electrophysiological studies. AM performed ultrasound and elastography studies on the patients and collected data. MM aided in analyzing the data and was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Patients were provided comprehensive trial information and the research was authorized by the Cairo University Ethics Board. Everyone who took part in the study gave their informed consent in writing. All research involving human participants in this study followed the guidelines established by the World Medical Association in their 1975 Declaration of Helsinki.
Consent for publication
All patients included in this research were fully conscious and older than 16-year old and gave written informed consent to publish the data contained within this study. I confirm that all contributors are in favor of submitting the work.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El-Shewi, I.EH., Tawfeek, A.A., Mohamed, A.A. et al. Role of conventional ultrasound and shear wave elastography of median nerve in diagnosis and differentiation of carpal tunnel syndrome severity in correlation with electrodiagnostic studies. Egypt J Radiol Nucl Med 55, 53 (2024). https://doi.org/10.1186/s43055-024-01215-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01215-0