- Research
- Open access
- Published:
Role of MRI in classification and preoperative evaluation of perianal fistula
Egyptian Journal of Radiology and Nuclear Medicine volume 55, Article number: 141 (2024)
Abstract
Background
A fistula is an unusual communication between the skin and an inward organ or between the organs. The current study aimed to determine the role of magnetic resonance imaging (MRI) in the diagnosis, description, and classification of fistula-in-ano. Additionally, the study aimed to compare the MRI findings with the operative findings, which is considered the gold standard in our study.
Methods
The present study is a prospective study and was carried out on a group of 61 patients: 52 males and 9 females with a mean age of 41 years, who were suspected to have perianal fistulae presented clinically with discharge or localized pain or were asymptomatic. A preoperative MRI was conducted for fistula-in-ano evaluation in these patients from October 2019 till the end of October 2021. A surgeon conducted a physical examination of all patients to document the number and location of cutaneous openings following a full medical history. The MRI images were evaluated and interpreted by multiple expert radiologists who had more than 5 years of experience in analyzing MRI. In the cases (in 3 cases, 4.92%) where there were discrepancies in their interpretations, a senior radiologist’s evaluation was considered the final result and was confirmed surgically. Subsequently, the MRI findings were correlated with surgical findings to indicate the specificity, sensitivity, and accuracy of such MRI findings.
Results
The MRI technique was the routine (i.e., without contrast administration) technique in 36 (59.02%) patients, with contrast administration in 21 (34.43%) patients and with anesthesia/sedation (uncomfortable, anxious, and claustrophobic patients need to minimize their motion artifact to improve the quality and obtain more detailed images) in 4 (6.56%) patients. The MRI pathology of the studied patients revealed normal findings in 1 (1.64%) patient, anal fissure/early developing tract in 6 (9.84%) patients, and established tract (sinus/fistula) in 54 (88.52%) patients. Park’s and St. James's University Hospital classifications were utilized to categorize the patients, with the most common fistula types based on the Park’s classification: intersphincteric (44.3%) and transsphincteric (29.5%). Based on the St. James’s classification, grade 1 (intersphincteric (34.4%)) and grade 4 (transsphincteric with abscess/side branch (16.4%)) were the most prevalent. A substantial consensus was reached between MRI and surgery findings for classifying tracts, side branches, and abscesses formation with sensitivity, specificity, and accuracy of 100%, 85.71%, and 98.36%, respectively.
Conclusions
MRI is a valuable tool in managing patients with perianal fistulas due to its ability to detect hidden areas of infection (such as abscesses) and secondary extensions. These factors contribute to the high recurrence rate after surgery. Additionally, MR imaging can define the anatomical relationships between the fistula and anal sphincters, helping to predict the likelihood of fecal incontinence following surgery.
Background
A perianal fistula (PAF) is an anomalous conduit connecting an anal canal entry point to an external cutaneous aperture in the perianal region. PAF is a common anorectal disorder in surgical practice, primarily affecting young adult males [1, 2].
The anal glands are situated in the intramuscular plane, at the level of the dentate line in the anal canal [3]. A high burden is imposed by anorectal sepsis [4]. Within the first year of an abscess presentation, persistent infection has the potential to propagate either circumferentially or axially, leading to the formation of a variety of fistulas [3, 4].
After hemorrhoids, fistula-in-ano ranks as the second most prevalent anorectal disorder [5]. In an effort to prevent a recurrence and maintain the functionality of the anal sphincter, surgery is the standard of care. Neglecting to identify and promptly excise a fistula and its associated components, including internal openings and secondary tracts, during surgery increases the possibility of recurrence to 25% [6,7,8]. Consequently, accurate preoperative evaluation of the fistulous tract is a critical diagnostic approach that significantly increases the surgical success rate.
Fistulography was employed to assess fistula-in-ano prior to the development of magnetic resonance imaging (MRI). Nevertheless, this modality exhibits a minimal diagnostic accuracy of approximately 16% and cannot visualize abscesses, secondary tracts, and sphincter complex owing to its inadequate contrast opacification [9]. Consequently, fistulograms are not capable of providing insights into the correlation between anal sphincters and fistula tracts. Endoanal ultrasonography is the initial imaging modality for visualizing anatomical structures within the anal canal [6]. In addition to abscesses and fistula-in-ano, it applies to the diagnosis and is utilized in treating prostate and anorectal tumors. Endoanal ultrasonography is remarkably advantageous in its ability to accurately identify primary fistulous tracts and internal apertures. [10, 11]. The limited field of vision is seen as a disadvantage of this modality, which undermines its effectiveness in assessing secondary tracts or supralevator extensions of a primary tract.
MRI has recently achieved significant recognition as the “gold standard” modality for the preoperative evaluation of fistula-in-ano. A precise and thorough evaluation that identifies primary tracks, ramifications, and abscesses is of the utmost importance in predicting surgical results and reducing complications, including recurrent lesions and fecal incontinence [6, 12, 13].
The current study aimed to determine the role of MRI in diagnosing, describing the characteristics, and classifying the types of fistula-in-ano, as well as the agreement between MRI and operative findings.
Methods
A cohort of 61 patients, with a mean age of 41 years, who were suspected to have PAF presented clinically with discharge or localized pain or were asymptomatic, participated in this prospective study.
Informed written consent was obtained from the patients. The study was conducted with the approval of the Diagnostic Medical Imaging and Intervention Radiology Department at the National Liver Institute-Menoufia University and the Radiology Department of Om El-Masreen General Hospital (Ministry of Health).
Inclusion criteria
Those criteria included patients who presented with a clinical picture of perianal discharge in most cases although local pain is also frequent; however, fistulas may be completely asymptomatic.
Exclusion criteria
Those criteria included patients who had absolute contraindications for undergoing an MRI scan. These contraindications include electronically and mechanically activated implants, ferromagnetic or electronically operated active devices such as automatic cardioverters, defibrillators, and cardiac pacemakers, metallic splinters in the eye, and ferromagnetic hemostatic clips in the central nervous system (CNS). Patients with renal impairment or contrast medium allergy prohibiting contrast medium administration and those undergoing radiotherapy or chemotherapy are relative contraindications for MRI scans.
Subjects
From October 2019 to the end of October 2021, images of patients who underwent preoperative MRI assessments as a preparation for surgical intervention for fistula-in-ano were collected. All patients underwent a physical examination by a surgeon to record the cutaneous openings (number and location) after a detailed medical history.
Patient preparation
No special patient preparation was performed. Prophylactic antihistaminic (Avil amp) and corticosteroids (Solucortif amp) were given to patients who received contrast media. Cases that need anesthesia/sedation (uncomfortable, anxious, and claustrophobic patients need to minimize their motion artifact to improve the quality and obtain more detailed images) fasted for 6 h.
MRI
It was conducted on a 1.5-T MRI unit, Philips (Achieva) and GE (Optima 450W GEM, Healthcare, Milwaukee, WI, USA). All the patients were imaged supine using a sense abdominal coil (XL Torso) (receive only coil).
Technique
Patients were imaged supine using an abdominal (XL Torso) coil. In comparison to a body coil, this method yields a superior signal-to-noise ratio, enhanced spatial resolution, and reduced imaging duration. The scan duration depends on the quantity of sequences employed. Each image sequence and plane require three to six minutes. Consequently, 15–30 min could be allotted for pelvic imaging in total.
Imaging field
In addition to encompassing the entire presacral space, the imaged volume must extend several centimeters above the levator ani muscle, both of which are frequent sites for extensions. Inclusion of the complete perineum is also recommended. Visualization of planes: Every patient underwent axial and coronal plane imaging.
MRI protocol
The sequences of acquired images included the following: axial FS T1W TSE, sagittal T2-weighted turbo spin-echo (T2W TSE), and oblique coronal fat-saturated (FS) T2W TSE; axial T1W TSE; axial FS T1W TSE; and oblique axial T2W TSE. After administering gadolinium intravenously at a rate of 0.2 ml/kg, post-contrast FS T1W TSE images were obtained in all three planes: sagittal, coronal, and axial. The sequence parameters utilized are detailed in Table 1.
MRI analysis
Independent interpretation and reporting were conducted on the images using picture archiving and communication system (PACS) by a group of radiologists, each with over 5 years of experience in MRI analysis. When there were disagreements regarding the interpretation (in 3 cases, 4.92%), the assessment of a senior radiologist was regarded as the ultimate determination.
The site of internal and external openings, the presence of secondary tracts or abscess formation, the location of primary tracts, and the existence of supralevator extension were assessed for each fistula-in-ano. The criteria established by Park's and St. James's University Hospital were used to classify fistulas [14, 15]. According to the criteria of Singh et al. and Torkzad et al. [16, 17] it was presumed that a fluid collection with rim enhancement on post-contrast T1W TSE images and a diameter greater than 10 mm was an abscess during image interpretation (Table 2).
The surgeon recorded the attributes of each fistula-in-ano during the operation and utilized this information to establish a correlation with the MRI results.
The PAF can be classified as follows:
-
(A)
Park’s Classification (subject to surgical interest; described the course and relationship of PAFs to the sphincter mechanism concerning coronal plane) [19, 20]: (1) An intersphincteric fistula traverses the intersphincteric space without traversing the external sphincter. (2) A transsphincteric fistula enters the ischiorectal fossa from the intersphincteric space, via the external sphincter, and descends into the fossa. (3) A suprasphincteric fistula ascends into the intersphincteric space and ascends above the puborectalis muscle before descending via the iliococcygeus muscle into the ischiorectal fossa and ultimately reaching the skin. (4) Lastly, an extrasphincteric fistula is not related to the internal or external anal sphincters.
-
(B)
Category of St. James’s University Hospital (subject to radiological interest; comprising abscesses and secondary extensions and determined by landmarks on the axial plane) [21]: Grade 1 is simple linear intersphincteric, grade 2 intersphincteric with abscess or secondary tract, grade 3 transsphincteric, grade 4 transsphincteric with abscess or secondary tract within the ischiorectal fossa, and grade 5 supralevator and translevator extension (Figs. 1, 2, 3, 4, 5 and 6)
Fig. 1 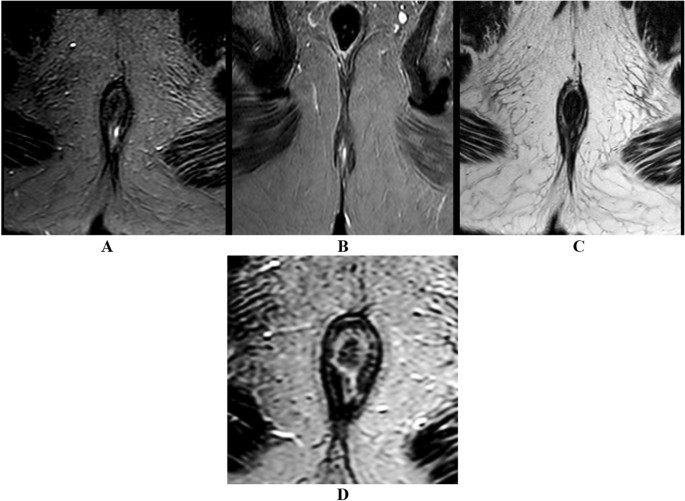
Axial STIR (A), coronal STIR (B), and axial T2 (C and D) images showing fluid-filled left perianal simple intersphincteric fistulas tract of bright T2/STIR signal seen connected to the internal anal sphincter at 5 o’clock position then descending downward within intersphincteric space to be ended by skin opening on the left aspect of the natal cleft
Fig. 2 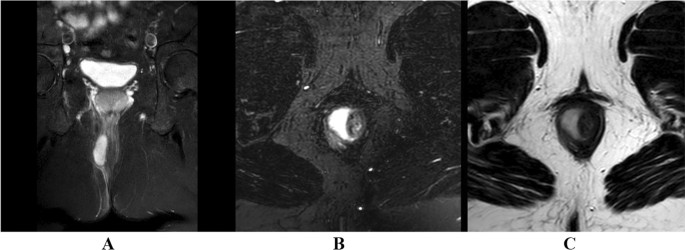
Coronal (A) and axial STIR (B) as well as axial T2 (C) images showing fluid-filled right perianal complex intersphincteric fistulas tract of bright T2/STIR signal seen connected to the internal anal sphincter at 6 o’clock position with localized collection seen within the right aspect of the intersphincteric space then the tract descending downward within intersphincteric space to be ended by skin opening on the right aspect of the natal cleft
Fig. 3 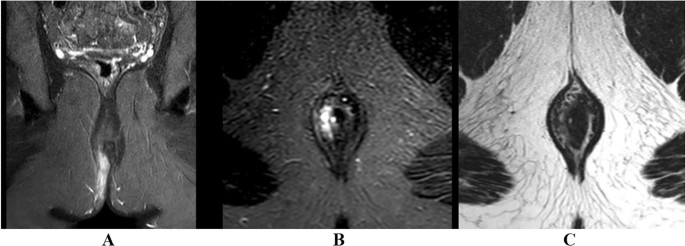
Coronal (A) and axial STIR (B) as well as axial T2 (C) images showing a fluid-filled right perianal complex intersphincteric fistulas tract of bright T2/STIR signal seen connected to the internal anal sphincter at 9 o’clock position with blind-ended intersphincteric side branch seen extended upward and anteriorly. The main tract descending downward within intersphincteric space is to end with a skin opening on the right aspect of the natal cleft
Fig. 4 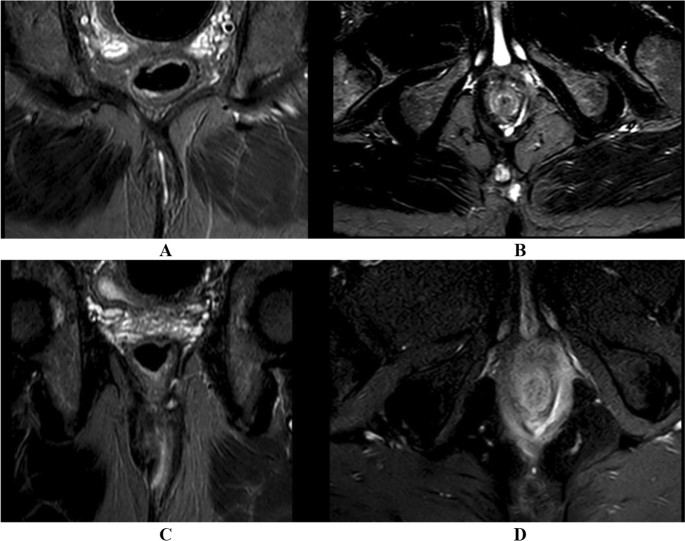
Coronal (A and C) and axial (B and D) STIR images showing fluid-filled left perianal complex transsphincteric fistulas tract of bright STIR signal seen connected to the internal anal sphincter at 6 o’clock position then passing within the intersphincteric plane giving left-sided blind ended intersphincteric side branch. The main tract also pierces the external anal sphincter at 5 o’clock position and then passes within the left ischioanal fossa slight left para-median in location to end with skin opening on the left aspect of the natal cleft
Fig. 5 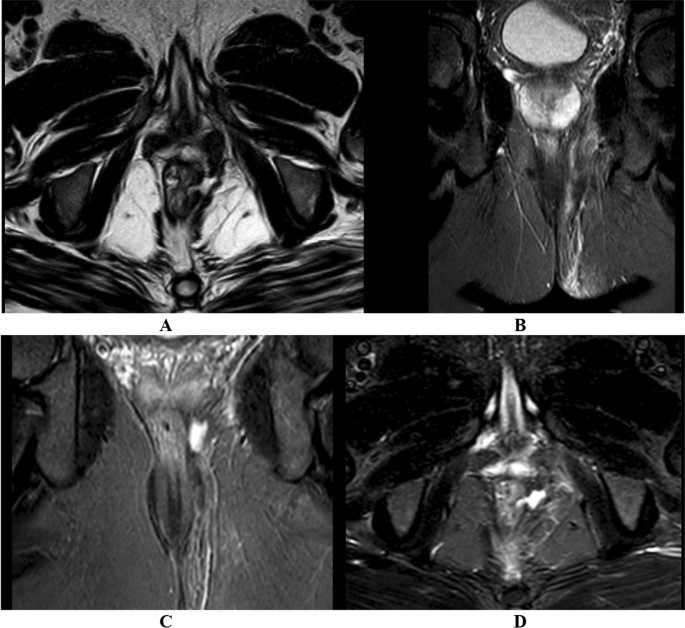
Axial T2 (A), coronal (B and C), and axial STIR (D) images illustrate a fluid-filled left perianal suprasphincteric/translevator fistulous tract with a bright T2/STIR signal connected to the left aspect of the lower rectal segment at 3 o’clock, with a small localized collection at the left ischiorectal fossa. The tract descends within the ischioanal fossa and terminates at a skin opening on the left
Fig. 6 
Sagittal (A), coronal (B), and axial (C) STIR images showing a fluid-filled pilonidal sinus of bright STIR signal seen at the slight left para-median retro-sacrococcygeal region extending from S2 level down to the uppermost part of the natal cleft being surrounded by subcutaneous edema and opening into the skin surface opposite S2 vertebra. It is seen infiltrating the deep retro-coccygeal region
.






Statistical analysis
For statistical analysis, SPSS v28 (IBM Inc., Armonk, NY, USA) was utilized. Frequency and percentage (%) representations of qualitative variables were employed for analysis using the Chi-square test. P values less than 0.05 with two tails were considered statistically significant.
Results
Regarding the baseline characteristics of the studied patients, there were 3 (4.92%) patients aged from 11 to 20 years, 8 (13.11%) patients aged from 21 to 30 years, 14 (22.95%) patients aged from 31 to 40 years, 26 (42.62%) patients aged from 41 to 50 years, 9 (14.75%) patients aged from 51 to 60 years, and 1 (1.64%) patient aged from 71 to 80 years. Patients less than 11 years, from 61 to 70 years, or more than 80 years were not included. The mean age was 41 years. 52 (85.25%) males and 9 (14.75%) females were included in our trial. The complaints of the studied patients were as follows: 55 (90.16%) patients had pain and discharge (for at least 6 months), and 6 (9.84%) patients had pain only. 10 (16.39%) of the studied patients had diabetes mellitus, 17 (27.87%) had hypertension, 1 (1.64%) had inflammatory bowel disease named Crohn’s disease, and 3 (4.92%) had hemorrhoids while 30 (49.18%) patients had no associations. All the studied patients had normal laboratory findings. Four (6.56%) of the studied patients underwent previous operative interference without preoperative MRI, no patient underwent previous operative interference with preoperative MRI, and 57 (93.44%) patients did not undergo any previous operative interference. The MRI technique was the routine (i.e., without contrast administration) technique in 36 (59.02%) patients, with contrast administration in 21 (34.43%) patients and with anesthesia/sedation (uncomfortable, anxious, and claustrophobic patients need to minimize their motion artifact to improve the quality and obtain more detailed images) in 4 (6.56%) patients. The MRI pathology of the studied patients revealed normal findings in 1 (1.64%) patient, anal fissure/early developing tract in 6 (9.84%) patients, and established tract (sinus/fistula) in 54 (88.52%) patients (Table 3).
Table 4 presents Park’s classification of the studied patients, where 7 (11.48%) patients had class 0 (no established fistula tract), 27 (44.26%) patients had class 1 (intersphincteric type), 18 (29.51%) patients had class 2 (transsphincteric), 3 (4.92%) patients had class 3 (suprasphincteric), 5 (8.2%) patients had class 4a (extrasphincteric (perianal sinus)), and 1 (1.64%) patient had class 4b (extrasphincteric (pilonidal sinus)). Table 4 also shows St. James's University Hospital classification of the studied patients, where 13 (21.31%) patients had grade 0 (no established fistula tract), 21 (34.43%) patients had grade 1 (simple intersphincteric with no abscess or side branch), 6 (9.84%) patients had grade 2 (intersphincteric with abscess or side branch), 8 (13.11%) patients had grade 3 (transsphincteric with no abscess or side branch), 10 (16.39%) patients had grade 4 (transsphincteric with abscess or side branch), and 3 (4.92%) patients had grade 5 (supralevator or translevator).
Among the studied patients, 12 (19.67%) patients had side branches, 12 (19.67%) had abscess formation, and 3 (4.92%) had supralevator extension (Table 5).
Table 6 displays the correlation between MRI findings and surgical findings (as a gold standard). Out of the 61 studied patients, 54 (88.52%) patients were confirmed surgically to have established tracks (true positive). There was a debate regarding 3 (4.92%) patients during their radiological interpretation, and the senior radiologist’s evaluation was considered the final result and confirmed surgically. Only 1 (1.64%) patient was suspected radiologically to have an early developing tract that was not detected/confirmed surgically (false positive). The remaining 6 (9.84%) patients had no tract (one of whom had a normal diagnosis while the others were diagnosed with anal fissures and confirmed clinically) which were confirmed surgically (true negative). The sensitivity, specificity, and accuracy of MRI in detecting anorectal fistula were 100%, 85.7%, and 98.4%, respectively.
The studied patients were followed up clinically at 1 week, 1 month, 3 months, and 6 months. Their outcomes were then classified as satisfactory (55 patients, 90.2%) or unsatisfactory (6 patients, 9.8%). Satisfactory outcomes mean that the patients did not require further surgery, experienced an improvement in their symptoms, and had a better quality of life. On the other hand, unsatisfactory outcomes mean that further surgery was necessary due to the recurrence of symptoms, fistula, and bad quality of life (Table 7).
There was a significant relation between grading of the patients according to Park's classification and complaint, inflammatory bowel disease association, MRI pathology (side branches, abscess formation), and outcomes (P < 0.05). There was an insignificant relation regarding sex, previous operative interference, and MRI technique, as illustrated in Table 8.
There was a significant relation between grading of the patients according to St. James's University Hospital classification and complaint, inflammatory bowel disease association, MRI pathology (side branches, abscess formation), and outcomes (P < 0.05). There was an insignificant relation regarding sex, previous operative interference, and MRI technique, as illustrated in Table 9.
Discussion
According to our research, the mean age of disease onset is 41 years, and the male-to-female ratio of PAFs in adulthood is approximately 6:1. These findings are consistent with the conclusions reached in previous investigations [16, 17, 22, 23].
The current study aimed to assess MRI accuracy in diagnosing, describing the characteristics, and classifying the fistula-in-ano types, as well as comparing MRI findings with operative results.
The present trial demonstrated that about 55 (90.16%) patients had pain and discharge, and 6 (9.84%) patients had pain only. There were no asymptomatic cases.
55 (84.6%) of the 65 patients surveyed by Algazzar et al. reported pain, whereas 10 patients (15.4%) did not. In addition, 18 patients (27.7%) exhibited perianal discharge, whereas 47 patients (72.3%) did not [24].
Anal glands were first related to fistula-in-ano by Chiari, who suggested that the glands were the source of infection (crypto-glandular theory). Currently, most studies agree with this hypothesis [25]. In our study, we found that idiopathic fistula-in-ano (with no associations or underlying cause) is the most common.
Spencer and colleagues [26] independently classified 37 patients into simple or complex fistulas (with the side branch, abscess formation, or with supralevator extension) based on MR imaging. Of the 37 patients, 22 (59%) had simple fistulas and 15 (41%) had complex fistulas. The present trial indicated that the MRI pathology of the studied patients revealed normal findings in 1 (1.64%) patient, anal fissure/early developing tract in 6 (9.84%) patients, and established tract (sinus/fistula) in 54 (88.52%) patients. About 12 (19.67%) patients had side branches, 12 (19.67%) had abscess formation, and 3 (4.92%) had supralevator extension.
Ano fistula classification according to Parks et al. [27], which was predicated on the tract's proximity to the anal sphincter muscle, was heavily criticized due to the hospital's particular characteristics and the omission of submucosal fistulas, which were superficial in nature and did not involve sphincteric structures [25].
Parks et al. [27], De Miguel et al. [28], Shoukat et al. [29], and Gage et al. [30] noted that intersphincteric fistula is the most common type (45%, 45%, 80% (24 out of 30 patients), and 54%, respectively). The second most common type is transsphincteric fistula (30%, 30%, 20% (6 out of 30 patients), and 21%, respectively). Parks et al. [27] found that suprasphincteric type is less common (20%) and the least common type is the extrasphincteric type (5%). De Miguel et al. [28] demonstrated that the least common type is extrasphincteric type (5%) and it is the only type that cannot be explained by crypto-glandular theory. Moreover, Gage et al. [30] illustrated that suprasphincteric and extrasphincteric are the least common (3%).
Our current trail indicated 7 (11.48%) unclassified patients (1 with normal MRI findings, 1 with suspected early developing submucosal tract, and 5 with anal fissure/focal mucosal inflammatory changes). The intersphincteric type is the most common type in 27 (44.26%) patients, and the second most common type is the transsphincteric type in 18 (29.51%) patients. Furthermore, we found the extrasphincteric type in 6 (9.8%) patients and the suprasphincteric type, which is the least common type, in 3 (4.92%) patients.
Morris et al. [18] revealed that the St. James's University Hospital classification (MR imaging-based classification) encompasses secondary ramifications and associated abscesses in addition to the demonstration of the primary fistulous track. Chaudhari et al. [31] discovered that grade I is the most prevalent type (18 (51%) out of 35 patients) and the second most common type is grade III (6 (21%) out of 35 patients). They also demonstrated that grade II (5 (14%) out of 35 patients) and grade IV (5 (14%) out of 35 patients) are less common and grade V (0 (0%)) is the least common type.
In our study, we found 13 (21.31%) unclassified patients (1 with normal MRI findings, 1 with suspected early developing submucosal tract, 5 with anal fissure/focal mucosal inflammatory changes, and 6 cases with perianal blind-ended sinus tracts not related anal sphincters). The most common type is grade I (21 (34.43%)), the second most common type is grade III (8 (13.11%)), the third common type is grade IV (10 (16.39%)), the fourth common type is grade III (8 (13.11%)), and the least common type is grade V (3 (4.92%)).
Singh et al. [32] reported that MRI accurately localized the internal opening and identified the fistula tract with a high degree of sensitivity (95.83%). Furthermore, Chauhan et al. [33] demonstrated that MRI had a remarkable sensitivity rate of 93.7% and a positive predictive value (PPV) of 96.7% when it was correlated with surgical findings.
Additionally, they determined that the sensitivity, specificity, PPV, NPV, and accuracy of MRI in representing the internal aperture were 98%, 85%, 99%, 85%, and 92%, respectively, using a comparable approach [34]. These findings are consistent with those of previous research and are anticipated.
In our study of 61 patients, 54 patients (88.52%) were confirmed surgically to have established tracks; there was a debate regarding 3 (4.92%) of such patients during their radiological interpretation, and the senior radiologist’s evaluation was considered the final result and confirmed surgically. Only one patient (1.64%) was suspected to have an early developing tract through the MRI, but it was not confirmed surgically. The remaining 6 patients (9.84%) did not have any tracts (one of them had normal MRI findings, while the others were diagnosed with anal fissures/focal inflammatory changes and confirmed clinically). Thus, the MRI sensitivity, specificity, accuracy, PPV, and NPV of our trail were 100%, 85.7%, 98.4%, 98.2%, and 100%, respectively.
Torkazad MR. et al. [35] demonstrated that this MR grading correlates with outcomes: grades one and two are associated with favorable outcomes (no recurrences, thus no reoperations are required), whereas grades three to five are associated with less favorable outcomes (recurrences necessitating reoperations).
The studied patients in our trial were followed up clinically for 6 months. Their outcomes were then classified as satisfactory (55 (90.2%) patients) or unsatisfactory (6 (9.8%) patients). Unsatisfactory outcomes are usually related to grades 3–5 in St. James’s University Hospital classification and related to grades 2 and 3 in Park's classification. Satisfactory outcomes mean that the patients did not require further surgery, experienced an improvement in their symptoms, and had a better quality of life. On the other hand, unsatisfactory outcomes mean that further surgery was necessary due to the recurrence of symptoms, fistula, and bad quality of life.
A significant relation (P < 0.05) was observed between Park's classification and MRI pathology (side branches, abscess formation) and outcomes (P < 0.05). Furthermore, a significant relation (P < 0.05) was observed between the St. James's University Hospital classification and MRI pathology (side branches, abscess formation) and outcomes.
In our study, MRI is an important diagnostic noninvasive tool for detecting primary fistulas, tract course, secondary tracts, or abscesses.
The fistulous tract's location and direction were delineated in our trail by employing an image of a clock face in the axial planes. We discovered that the fistulous tracks are accurately depicted in the coronal and axial planes in relation to the sphincter complex, ischiorectal fossa, and levator plate. Transsphincteric fistulas are distinguished from intersphincteric fistulas by the presence of disruption of the external anal sphincter [36]. Lastly, the levator ani's integrity should be examined to determine the presence of suprasphincteric or translevator disease. The coronal plane is the most effective method for detecting levator ani affection in our study.
Our trail indicates that radiologists interpreting the MRI examination should provide a description of the fistula tract's relationship to the sphincter complex as well as the location of the internal and external openings. The internal aperture can be delineated using the “anal clock” feature implemented in axial MRI.
As in the trail conducted by Torkazad MR. et al. [35] and Singh et al. [32], It was presumpted that a fluid collection exceeding 10 mm was classified as an abscess, while a fluid-filled tubular structure less than 10 mm was classified as a fistula tract. Singh et al. [32] detected 7 out of 50 cases with abscesses, but in our study we found about 12 (19.67%) patients with abscesses and 12 (19.67%) with side branches.
Recommendations
-
MRI is highly recommended as the preferred diagnostic noninvasive imaging modality for preoperative assessment of PAF. This can significantly reduce the chances of recurrence and the need for further surgical intervention, ultimately improving the patient's quality of life.
-
Intravenous contrast MRI can be omitted, especially when assessing primary or previously unoperated PAF.
Limitations
-
The high cost of the scan and availability of MRI are among the limitations in our study. However, the statistically significant relation (P < 0.05) among the MRI classification and clinical outcomes of the studied patients improved its cost-effectiveness in the long term.
-
The sample size (n = 61) was small and from only two centers, affecting the results as follows:
-
1.
The error rate increased with subsequent low statistical power.
-
2.
The small differences among the groups in small samples may lead to statistically insignificant results.
-
3.
Non-normal distribution may occur.
-
These limitations were due to our trail being prospective, and all patients were followed up for at least 6 months after surgical intervention, making the long-term follow-up for a larger sample size difficult and costly.
-
We propose that to validate and generalize our findings, a larger sample size be obtained through multicenter collaboration.
Conclusions
MRI is a valuable tool in managing patients with perianal fistulas due to its ability to detect hidden areas of infection (such as abscesses) and secondary extensions. These factors contribute to the high recurrence rate after surgery. Additionally, MR imaging can define the anatomical relationships between the fistula and anal sphincters, helping to predict the likelihood of fecal incontinence following surgery.
Availability of data and materials
The datasets used and analyzed during the current study are available upon reasonable request from the corresponding author Mohamed Badr.
Abbreviations
- 3D US:
-
Three-dimensional ultrasonography
- ADC:
-
Apparent diffusion coefficient
- CE:
-
Contrast enhanced
- CNS:
-
Central nervous system
- DW:
-
Diffusion-weighted imaging
- FOV:
-
Field of view
- FS:
-
Fat-saturation pulse sequence
- IV:
-
Intravenous
- MRI:
-
Magnetic resonance imaging
- NPV:
-
Negative predictive value
- PAF:
-
Perianal fistula
- PPV:
-
Positive predictive value
- STIR:
-
Short tau inversion recovery pulse sequence
- T:
-
Tesla
References
Igwe PO, Dodiyi-Manuel A, Oparaku KC (2014) The pattern of surgically treatable anorectal diseases in University of Port Harcourt Teaching Hospital, Rivers State, Nigeria. Niger J Med 23(1):57–60
Algazzar HY, Eldib DB, Bahram MA, Zaher NA (2019) Preoperative MRI of perianal fistula evaluation and its impact on surgical outcome. Egypt J Radiol Nucl med 50(2):1–10
Abeysuriya V, Salgado LS, Samarasekera DN (2010) The distribution of the anal glands and the variable regional occurrence of fistula-in-ano: is there a relationship? Tech Coloproctol 14(4):317–321
Sahnan K, Askari A, Adegbola SO, Tozer PJ, Phillips RKS, Hart A et al (2017) Natural history of anorectal sepsis. Br J Surg 104(13):1857–1865
Nguyen DH (2007) Gastrointestinal surgical treatment. In: Nguyen DH (ed) Medical Publishing House, pp 191–217
de Miguel Criado J et al (2012) MR imaging evaluation of perianal fistulas: spectrum of imaging features. Radiograph: Rev Publ Radiol Soc North Am, Inc 32:175–194. https://doi.org/10.1148/rg.321115040
Do DC (2007) The reasons of failure in surgery for anal fistula. Ho Chi Minh City Med J 11:177–179
Lilius HG (1968) Fistula-in-ano, an investigation of human foetal anal ducts and intramuscular glands and a clinical of 150 patients. Acta Chir Scand Suppl 383:7–88
Kuijpers HC, Schulpen T (1985) Fistulography for fistula-in-ano. Is it useful? Dis Colon Rectum 28:103–104. https://doi.org/10.1007/bf02552656
Buchanan GN et al (2004) Clinical examination, endosonography, and MR imaging in preoperative assessment of fistula in ano: comparison with outcome-based reference standard. Radiology 233:674–681. https://doi.org/10.1148/radiol.2333031724
Vo TD, Nguyen QTD (2007) Endorectal ultrasonography with hydrogen peroxide in diagnosis of anal fistulas and ano-vaginal fistulas. Ho Chi Minh City Med J 11:17–23
Agha ME, Eid M, Mansy H, Matarawy K, Wally M (2013) Preoperative MRI of perianal fistula: Is it really indispensable? Can it be deceptive? Alex J Med 49:133–144. https://doi.org/10.1016/j.ajme.2012.09.003
Konan A, Onur MR, Özmen MN (2018) The contribution of preoperative MRI to the surgical management of anal fistulas. Diagn Interv Radiol 24:321. https://doi.org/10.5152/dir.2018.18340
Parks A, Gordon PH, Hardcastle J (1976) A classification of fistula-in-ano. Br J Surg 63:1–12. https://doi.org/10.1002/bjs.1800630102
Morris J, Spencer JA, Ambrose NS (2000) MR imaging classification of perianal fistulas and its implications for patient management. Radiograph: Rev Publ Radiol Soc North Am, Inc 20:623–635. https://doi.org/10.1148/radiographics.20.3.g00mc15623
Singh K, Singh N, Thukral C, Singh KP, Bhalla V (2014) Magnetic resonance imaging (MRI) evaluation of perianal fistulae with surgical correlation. J Clin Diagn Res: JCDR 8:RC01
Torkzad MR, Ahlström H, Karlbom U (2014) Comparison of different magnetic resonance imaging sequences for assessment of fistula-in-ano. World J Radiol 6:203. https://doi.org/10.4329/wjr.v6.i5.203
Morris J, Spencer A, Ambrose N (2000) MR imaging classification of perianal fistulas and its implications for patient management. Radiographic 20(3):623–635
Parks AG (1961) Pathogenesis and treatment of fistula-in-ano. Br Med J 1(5):463–469
de Miguel Criado J, del Salto LG, Rivas PF, del Hoyo LF, Velasco LG, de las Vacas MI et al (2012) MR imaging evaluation of perianal fistulas: spectrum of imaging features. Radiograph 32(1):175–194
Morris J, Spencer JA, Ambrose NS (2000) MR imaging classification of perianal fistulas and its implications for patient management. Radiographics 20(3):623–637
Abcarian H (2014) Anal fistula: principles and management. In: Abcarian H (ed), Springer, pp 13–32
Buchanan G et al (2002) Effect of MRI on clinical outcome of recurrent fistula-in-ano. The Lancet 360:1661–1662. https://doi.org/10.1016/S0140-6736(02)11605-9
Algazzar HY, Eldib DB, Bahram MA, Zaher NA (2019) Preoperative MRI of perianal fistula evaluation and its impact on surgical outcome. Egypt J Radiol Nucl Med 50:1–10
Szurowska E, Wypych J, Izycka-Swieszewska E (2007) Perianal fistulas in Crohn’s disease:MRI diagnosis and surgical planning. Abdom Imag 32(6):705–718
Spencer JA, Chapple K, Wilson D et al (1998) Outcome after surgery for perianal fistula: predictive value of MR imaging. AJR Am J Roentgenol 171:403–406
Parks AG, Gordon PH, Hardcastle JD (1976) A classification of fistula- in-ano. Br J Surg 63(1):1–12
De Miguel CJ, Garcia del Salto L, Rivas PF et al (2012) MR imaging evaluation of perianal fistulas: spectrum of imaging features. Radiographics 32:175–194
Shoukat S, Bux K, Nisar H et al (2016) Pre-operative MRI Evaluation of fistula in ano. Pak J Radiol 26(3):198–201
Gage KL, Deshmukh S, Macura KJ et al (2013) MRI of perianal fistulas: bridging the radiological–surgical divide. Abdom Imag 38(5):1033–1042
Chaudhari NH, Sinkar AD, Swoyam S (2016) Role of magnetic resonance imaging in evaluation of perianal fistulas. Int J Res Med Sci 4(2):482–485
Singh K, Singh N, Thukral C, Singh KP, Bhalla V (2014) Magnetic resonance imaging (MRI) evaluation of perianal fistulae with surgical correlation. J Clin Diagn Res 8(6):1–13
Chauhan NS, Sood D, Shukla A (2016) Magnetic resonance imaging (MRI) characterization of perianal fistulous disease in a rural-based tertiary hospital of North India. Pol J Radiol 81(6):611–622
Vo D, Phan C, Nguyen L, Le H, Nguyen T, Pham H (2019) The role of magnetic resonance imaging in the preoperative evaluation of anal fistulas. Sci Rep 9(1):17947–17955
Torkzad MR, Karlbom U (2010) MRI for assessment of anal fistula. Insights Imag 1(2):62–71
O’Malley RB, Al-Hawary MM, Kaza RK et al (2012) Rectal imaging: part 2 perianal fistula evaluation on pelvic MRI-what the radiologist needs to know. AJR Am Roengenol 199:W43-53
Acknowledgements
Many thanks to all the staff members who helped us to finish our study.
Funding
None to be declared.
Author information
Authors and Affiliations
Contributions
All authors co-operated in work design, creation of data, detection of resources, data interpretation, validation, and methodology, writing draft and revision. All authors provided comments on the manuscript at various stages. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
It was approved by the Institutional Review Board of the National Liver Institute (NLI IRB number 00014014), Menoufia University. An informed written consent was obtained from the participants. The study was conducted from October 2019 till the end of October 2021.
Consent for publication
All patients included in this study gave informed consent to publish the data contained within this study.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Aly, R.A., Badr, M.A., Korayem, E.M. et al. Role of MRI in classification and preoperative evaluation of perianal fistula. Egypt J Radiol Nucl Med 55, 141 (2024). https://doi.org/10.1186/s43055-024-01304-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01304-0