- Research
- Open access
- Published:
Additive role of dynamic subtraction MRI in assessment of unresolved HCC post-radiofrequency ablation
Egyptian Journal of Radiology and Nuclear Medicine volume 52, Article number: 257 (2021)
Abstract
Background
Malignant Hepatocellular carcinoma (HCC) is one amongst the foremost widespread cancers within the world. Radiofrequency ablation (RFA) is that the most generally used substitute tool for hepatic carcinoma treatment. Monitoring tumoral response to loco-regional therapy is a vital mission in oncological imaging. Dynamic contrast enhanced MR and recently added subtraction imaging technique improve assessment of the ablated hepatic focal lesions. The aim of this study is that the evaluation of the role of Subtraction MRI within the detection of recurrent or residual tumoral viability after RF ablation.
Results
Fifty patients were conducted during this retrospective study, all underwent RFA for 76 hepatic focal lesions and underwent Dynamic MRI study 1 month after ablation. Subtraction imaging was then performed. MRI images were interpreted by two readers who are experienced in hepatic imaging. The primary reader interpreted the standard Dynamic MRI and was blinded to the subtraction sequences; the second reader interpreted both Dynamic and Subtraction MRI images. the primary reader detected 49 resolved cases by dynamic MRI, while the second reader detected residual activity in 6 cases out of 49 via subtraction dynamic MRI (added value). The second reader agreed with first reader in 43 cases (agreement).The first reader detected 27 residual cases by dynamic MRI. The second reader disagreed with first reader in 11 cases appeared resolved out of 27 via subtraction dynamic MRI (added value). The second reader agreed with first reader in residual activity in 16 cases (agreement).The statistical analysis of those results revealed a big additive value of the subtraction imaging to the dynamic MRI (P < 0.001) with moderate degree of agreement between the 2 diagnostic tools (Kappa value = 0.491). This implies that Subtraction MRI significantly improves the reader confidence level within the assessment of treatment response following loco-regional therapies for HCC.
Conclusion
Dynamic Subtraction MRI is a powerful detector for real enhancement in treated HCC lesions after radiofrequency ablation and hence increasing the degree of readers’ confidence and accuracy of treated lesions in follow-up studies. So it's recommended to feature this powerful tool as a routine to any or all Dynamic MRI studies of the Liver.
Background
Hepatocellular carcinoma (HCC) is one in all the foremost widespread cancers within the world, and incorporates a poor prognosis unless treated. Patients with liver cirrhosis are at highest risk of developing malignant disease [1].
The gold standard therapy for HCC is surgical resection. However, unfortunately; only 10–15% of HCC patients are suitable for resection because of the severity of underlying cirrhosis or the diffuse distribution of the tumor. Liver transplantation is theoretically the simplest treatment for HCC. Several minimally invasive techniques are used as alternatives to surgery for hepatic cancer treatment, including percutaneous RFA [2].
Thermal ablation is achieved by using either heat (radiofrequency ablation, microwave ablation, laser ablation); or cold (cryoablation). RF ablation is that the one most generally used thermal ablation techniques for both primary and secondary malignances of the liver, yet all techniques produce coagulation necrosis, and demonstrate similar imaging features on follow-up studies [3].
Monitoring tumor response to loco-regional therapy is incredibly important in oncological imaging. Early good response indicates therapy effectiveness, and will lead to significant survival benefit. Early detection of treatment failure is critical in patient management, since treatment repeated cycle will be performed if liver functions are maintained, before disease progression occurs [4].
New advances in functional imaging techniques have provided the aptitude of detection of microscopic changes in tumor micro-environment and micro-structure, allowing the assessment of tumor response after loco-regional treatment by observing alterations in tumor viability, perfusion or vascularity [5].
The change in tumor vascularity and perfusion after frequency ablation will be assessed by dynamic contrast enhanced MR imaging. Subtraction and color mapping were also improved to guage the ablated hepatic lesions [5].
The treated lesion exhibits high signal intensity on T1-weighted images [6]. Hence, subtraction imaging are helpful to assess the therapeutic efficacy for RF Ablation for HCCs where after which coagulative necrosis usually occur exhibiting bright T1 signal which makes the detection of tumor enhancement difficult on post-contrast T1-weighted images [7].
Subtraction is an automatic process present on the software of most of the recent MR scanners in addition as their workstations. That does not need any extra-time during image acquisition because it could be a post processing technique not a picture sequence [8].
By accomplishing this operation, any native T1 signal is masked and the remaining signal on the subtracted images is simply because of enhancement [7] (Fig. 1).

Schematic diagram illustrating the principles of subtraction MRI in treatment zones of varying characteristics [7]
Methods
Patients
A retrospective study was performed on 50 cases of HCC who underwent radiofrequency over a period of 12 months. The study was conducted in a private radiology center over period of 12 month. The patients’ ages ranged between 40 to 74 years. All patients signed a written consent before the MRI examination.
Inclusion criteria
HCC patients underwent RFA procedure as the only therapeutic intervention.
Exclusion criteria
-
Contraindications to magnetic resonance imaging, e.g. claustrophobia, cardiac, pacemakers, Brain coils
-
Tumors other than hepatocellular carcinoma
All cases had been subjected to the following:
-
Full clinical data.
-
Viewing the patient's laboratory investigations including renal function tests (urea and creatinine).
-
Viewing the previous radiological investigations done for the patients.
-
Patients were scheduled to undergo MRI 1 month after ablation.
Methods
MRI protocol
Cases were performed using Philips 1.5 Tesla MRI scanner (Achieva).
-
(a)
Pre-contrast imaging
Sequence
TR (msec)
TE (msec)
FOV (mm)
Flip angle
Slice thickness
1 T
1.5 T
1 T
1.5 T
1 T
1.5 T
1 T
1.5 T
1 T
1.5 T
Axial T1 TFE
14
10
6.9
4.6
300–350
15
15
7 mm
Axial T2 TSE
1000
1000
80
80
300–350
90
90
7 mm
Axial T2 SPAIR
1000
1000
80
80
300–350
90
90
7 mm
-
(b)
Diffusion study
-
Diffusion MR imaging was performed before the dynamic study using respiratory triggered fat-suppressed single-shot spin echo echoplanar sequence that combined the two diffusion (motion-probing) gradients before and after the 180° pulse.
-
The acquisition parameters for 1 Tesla machines were: TR 2270 ms, TE 78 ms, matrix 100 × 83 with a field of view as small as possible, slice thickness 10 mm, slice gap 1–2 mm, scan time 4–5 min. We used b values of 0, 400 and 800 s/mm2.
-
The acquisition parameters for 1.5 Tesla machines were: TR 1700 ms, TE 76 ms,matrix 120 × 95 with a field of view as small as possible, slice thickness 10 mm, slice gap 1–2 mm, scan time 3–4 min. We used b values of 0, 500 and 1000 s/mm2.
-
-
(c)
Dynamic study
-
Dynamic study was performed after manual bolus injection of 0.1 mmol/kg body weight of Gd-DTPA.
-
Dynamic imaging using3D fat-suppressed T1-weighted gradient echo sequence (THRIVE i.e. T1 high-resolution isotropic volume examination). A dynamic series consisted of one pre-contrast series followed by four successive post-contrast series including early arterial, late arterial, and portal phases with 19–21 s intervals (17 s for image acquisition with breath-holding and 2–4 s for re-breathing)this is followed by 5-min delayed phase imaging. All patients were imaged in end expiration to limit the risk of image misregistration.
-
Acquisition parameters for open 1 Tesla machine were TR 3.3 ms., TE 1.6 ms, flip angle 10°, matrix size, 136 × 108, field of view 300–350 mm and slice thickness 2–3 mm.
-
Acquisition parameters for 1.5 Tesla machines were TR 4.4 ms, TE 2.1 ms, flip angle 10°, matrix size, 172 × 163, field of view 300–350 mm and slice thickness 2–3 mm.
-
Analysis of the MR images
-
Images were sent to the workstation (Phillips Extended MR Workspace) for further image processing.
-
The morphological features of each lesion were recorded including size, border and signal intensity at T1, T2 and SPAIR images.
-
Assessment for the presence of residual or recurrent tumor viability.
-
Dynamic study analysis We perform early arterial, late arterial, portal and delayed phases after the single pre-contrast series. Pattern of enhancement (through the successive Dynamic series) was hen studied.
-
Subtraction dynamic study analysis Subtraction imaging was then performed which is automated process available on the workstation, whereby an unenhanced T1-weighted sequence is digitally subtracted from the identical sequence performed after gadolinium administration. In our study the pre-contrast series was digitally subtracted from the late arterial phase in the dynamic study. By performing this operation, any native T1 signal is removed and the remaining signal on the subtracted images is due solely to enhancement.
-
Pattern of enhancement in the subtraction dynamic imaging were then studied.
Interpretation of the MR image
MR images were interpreted by two readers of more than 10 years’ experience in hepatic imaging, each read the films separately, yet both had the clinical data of the patients. The first reader interpreted the Dynamic MRI and was blinded to the subtraction MRI images; the second reader interpreted both Dynamic and Subtraction MRI images.
Signal of the ablation zone at T1, T2 and SPAIR WIs was classified as: high, low or heterogenous.
-
A.
Dynamic study interpretation by the first reader:
-
Arterial phase enhancement and delayed wash out were recorded and suggesting residual tumoral activity.
-
Absence of enhancement in the arterial phase was recorded and suggested well tumor ablation.
-
-
B.
Dynamic and subtraction dynamic studies interpretation by the second reader:
-
The second reader also interpreted the Dynamic study to detect enhancing lesion on the arterial phase that suggested residual tumor activity
-
Contrast wash out: Decrease in the enhancement on delayed phase imaging compared with early phase imaging.
-
Then recorded findings were confirmed/corrected by the subtraction images to prove that the high signal in the arterial phase is due to enhancement and not due to the original precontrast high T1 signal of the coagulative necrosis.
-
Interpretation of the presence of ill-defined perilesional parenchymal enhancement
-
Post-interventional reactive changes: this is defined as early phase enhancement beyond the ablated cavity on the surrounding liver parenchyma that persists in the delayed phase.
-
Perfusion abnormalities (transient hepatic intensity difference): ill-defined parenchymal enhancement during the arterial phase. This occurs in cases of injury of the portal vein or traumatic arterio-portal shunting.
-
Well-defined enhancement at the margin of the ablation zone which may be either:
-
Granulation tissue rim: persistent or delayed phase enhancement.
-
Nodular or hallow enhancement: that suggest tumor recurrence.
-
Pattern of enhancement impressive for tumor progression
We follow the classification reported by Chopra et al. as follow:
-
Halo type: irregular, thick rim of enhancement around the ablation zone.
-
Nodular type: nodular foci of enhancement at the margins of the treated ablation zone.
-
Gross enlargement type: overall increase in the size of the treated zone.
We studied the signal intensity of the entire Ablation zone in the non-enhanced T1 and T2 images classified into the following:
-
1.
Heterogeneous high signal.
-
2.
High signal.
-
3.
Iso-intense/intermediate signal.
-
4.
Hypointense signal.
We also studied the frequency distribution of T1 and T2 signals in unresolved and resolved lesions based on subtraction MRI findings.
Statistical methods
Data management and statistical analysis were done using SPSS vs.25. Numerical data was summarized using means and standard deviations or medians and ranges. Categorical data was summarized using numbers and percentages. Categorical data was compared between resolved and unresolved lesion—based on subtraction MRI—using Chi-square test. Kappa coefficient was calculated to indicate degree of agreement between conventional MRI and Dynamic MRI. Kappa coefficient of 0 indicates no agreement while kappa coefficient of 1 indicates perfect agreement. Diagnostic indices including sensitivity, specificity, PPV and NPV were calculated for conventional MRI and diffusion MRI using subtraction as a gold standard. All P values were two sided. P value less than 0.05 was considered significant.
Results
The first and second readers agreed in their results while reviewing the dynamic MRI images, the difference in results between the two readers appeared after the second reader added the value of subtraction images to the dynamic MRI images hence correcting the opinion.
-
A.
The dynamic MRI imaging (first reader) 48 (63%) lesions were
Resolved (well-ablated) lesions while 28 (37%) lesions showed recurrent/residual viability.
-
B.
The subtraction dynamic MRI imaging (second reader) 54 (71%)
Lesions were all found to be resolved (well-ablated) while 22 (28%) lesions showed recurrent / residual viability.
-
C.
Correlation between findings of first reader and second reader: (Table 1; Fig. 2)
-
The well ablated (resolved) lesions:
-
The first reader detected 49 resolved cases by dynamic MRI while the second reader detected residual activity in 6 cases out of 49 via subtraction dynamic MRI.
-
The second reader agreed with first reader in 43 cases.
-
-
The well ablated (resolved) lesions:
-
The first reader detected 49 resolved cases by dynamic MRI while the second reader detected residual activity in 6 cases out of 49 via subtraction dynamic MRI.
-
The second reader agreed with first reader in 43 cases.
-
-
The residual (unresolved) lesions:
-
The first reader detected 27 residual cases by dynamic MRI
-
The second reader disagreed with first reader in 11 cases appeared resolved out of 27 via subtraction dynamic MRI
-
The second reader agreed with first reader in residual activity in 16 cases.
-
The statistical analysis of these results revealed a significant additive value of the subtraction imaging to the dynamic MRI (P < 0.001) with moderate degree of agreement between the two diagnostic tools (Kappa value = 0.491). This means that Subtraction MRI significantly improves the reader Confidence level in the assessment of treatment response following locoregional therapies for HCC (Table 2).
-
-
D.
We studied the T1 Signal in the Entire Ablation Zone, we found that Within the treated 76 lesions imaged after RF Ablation; 48 Leisons (63.2%) showed Hyperintense signal, 24 Lesions (31.6%) showed heterogenous signal and 4 Lesions (5.3%)showed hypointense signal (Fig. 3).
Treated lesions exhibits high signal intensity on T1-weighted images. Hepatic lesions treated with RFA and showed very high T1 signal was detected. RF treated areas were hypo-intense and homogeneous at unenhanced T1-weighted MR images or were high heterogeneous with a peripheral hyper-intense ring. (Table 3).
D- Correlation between the T2 signal intensity of the ablated zone and the residual tumor activity / recurrent neoplastic viability via statistical analytic view: Data were analyzed using Chi-square test / Fisher’s exact test. No Significant correlation between the T2 signal intensity and neoplastic Viability was detected (Table 4).

The degree of agreement between the two readers and the additive value of subtraction technique to the dynamic MRI study

Pie Chart showing the signal intensity of the entire ablation zone in the non-enhanced T1 images
We assessed the Diffusion Pattern of all Lesions Residual and Resolved in relation to the added Subtraction Dynamic MRI Technique as a Gold Standard:
-
We found that out of 54 Resolved lesions; 48 lesions (88.9%) showed No Restriction and only 6 (11.1%) lesions showed Restriction
-
We Also founded that out of 22 unresolved/Residual lesions; 15 lesions (68.2%) showed Restriction and 7 (31.8%) lesions showed No Restriction (Fig. 4; Table 5).
Fig. 4 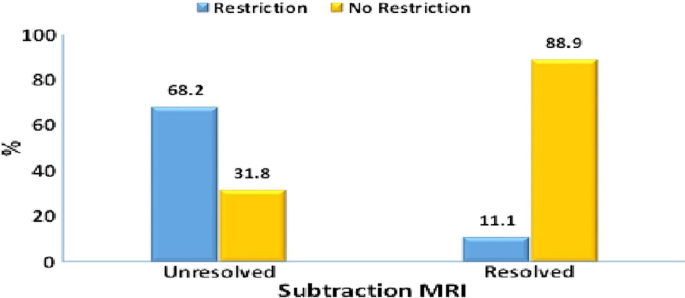
A chart assessing the diffusion pattern of all lesions residual and resolved in relation to the added subtraction dynamic MRI technique as a gold standard

Compared to DWI, Subtraction MRI is much more valuable, where it increase radiologists’ confidence in interpreting treatment response following loco-regional therapies for HCC based on a in a study on 32 patients with 54 HCC lesion that compared Subtraction MRI versus diffusion weighted imaging in post locoregional treatment of HCC, where Diffusion WI MRI showed Sensitivity 70.6%, Specificity 75%, PPV 82.7% and NPV 60% compared to Added Subtraction Dynamic MRI with sensitivity 97%, specificity 100%, PPV 100% and NPV 95%.
Discussion
Hepatocellular carcinoma (HCC) is one of the foremost common cancers worldwide, and encompasses a poor prognosis if not treated. Cirrhotic patients are at highest risk of developing this malignant disease [1].
Generally, surgical resection and liver transplantation are the most effective treatment decision for HCC But unfortunately; only 10–15% of HCC patients are eligible for resection because of the severity of underlying cirrhosis or the diffuse distribution of the tumor and absence of donor organs hinder both options so several minimally invasive techniques are used as alternatives to surgery for treating the disease and one amongst widely used is percutaneous radio-frequency ablation [2].
Thermal ablation is achieved by using heat (radiofrequency ablation, microwave ablation, laser ablation); or cold (cryoablation). Among all the ablative techniques, RF ablation is that the one most generally used for treatment of carcinoma, but all techniques produce coagulation necrosis, and demonstrate similar imaging features on follow-up studies [3].
Monitoring tumor response to loco-regional therapy is an increasingly important task in oncologic imaging. Early favorable response generally indicates effectiveness of therapy, and will lead to significant survival benefit. Early identification of treatment failure is additionally critical in patient management, since a repeat treatment cycle is performed if liver function is maintained, before disease progression occurs [4].
Recent advances within the development of functional imaging techniques have provided the power to detect microscopic changes in tumor microenvironment and microstructure, thus allowing the assessment of tumor response after locoregional treatment by observing alterations in tumor viability, perfusion or vascularity [5].
Dynamic contrast enhanced MR imaging can assess the change in tumor vascularity and perfusion after ablation. Recently, Subtraction and color mapping were developed to boost the evaluation of the ablated hepatic lesions [6].
Subtraction imaging relies on removing any preexisting signal of T1 unenhanced images causing contrast enhancement within a mass to become more conspicuous on subtracted sequences. This can be helpful when evaluating a lesion with high signal on unenhanced T1-weighted sequences, where visual detection of the enhancement is difficult on conventional MR [7].
Our findings agreed with Kierans et al. [9] who demonstrated that the treated lesions exhibits high signal intensity on T1-weighted images.
In our study, the T2 signal was variable in Treated ( Ablation Zone), Within the treated 76 lesions; 41Leisons (53.9%) showed Intermediate/Iso intense signal, 16 Leisons (21.1%) showed heterogeneous signal and 13 Lesions (17.1%)showed hypointense signal and only 6 Lesions (7.9%) showed hyperintense signal.
These findings agreed with Hussein et al. [10], that also found also variable T2 signal intensity. They explained the high signal by the liquifactive necrosis, which occurs late, and therefore the low signal by the coagulative necrosis which occurs early.
We did a statistical analysis to detect any relationship between the T2 signal and also the tumor viability. We found there's no significant difference within the signal intensity of the whole ablation zone between the resolved and unresolved lesions at the first follow up imaging. These findings agreed with Granata et al. [11] who also didn't detect any significant correlation between the T2 signal and neoplastic activity.
On the opposite hand, Hussein et al. [10] found 86% of RF treated areas to be homogeneous hypo intense signal on T2 weighted images thanks to coagulative necrosis while only 14% showed markedly high heterogeneous signal intensity thanks to liquifactive necrosis. The superior sensitivity of T2-weighted imaging might be explained by a rise in contrast between the coagulated area that features a low signal intensity, and also the viable residual tumor which includes a high signal intensity. Moderate hyperintensity on T2-weighted images corresponded to the presence of residual viable tumor altogether cases. Therefore, T2-weighted imaging is demonstrated to be highly specific. Moreover, the moderately hyperintense area on T2-weighted images related to corresponding enhancement on contrast-enhanced T1-weighted images offers optimal specificity (100%) for residual viable tumor all told cases.
In our study, we found a relation between the pre-contrast T1 signal intensity and therefore the mismatched findings between the primary and second readers where we noticed that the mismatch occurs in cases with high T1 signal intensity in pre-contrast series.
Winters et al. [12] agreed with our study regarding the relation between precontrast signal and interpretation of imaging where they found that the Treated ablated zones show high signal on the unenhanced T1-weighted images secondary to coagulative hemorrhagic necrosis that complicates the interpretation of contrast- enhanced MRI. The contrast-enhanced T1-weighted high signal is also a results of enhancement, pre-existing T1-weighted high signal, or a mix of those and hence the issue in interpretation.
We compared statistical analysis between Conventional Dynamic MRI in addition because the Diffusion WI ends up in respect to added value of Subtraction MRI, as a gold standard, We found that adding diffusion MRI can provide more accuracy to plain conventional Dynamic MRI increased Specificity and Positive Predictive values.
The findings nearly matched with those findings in an exceedingly study performed by Hamed et al. [13] that concluded that Compared to DWI, Subtraction MRI is way more valuable, where it increases radiologists’ confidence in interpreting treatment response following loco-regional therapies for HCC supported a in an exceedingly study on 32 patients with 54 HCC lesion that compared Subtraction MRI versus diffusion weighted imaging in post locoregional treatment of HCC, where Diffusion WI MRI showed Sensitivity 70.6%, Specificity 75%, PPV 82.7% and NPV 60% compared to Added Subtraction Dynamic MRI with Sensitivity 97%, Specificity 100%, PPV 100% and NPV 95%.
In our study and on revising the info collected from both readers we noted that the subtraction technique has an additive value plus the agreement with the dynamic technique. These results revealed a big additive value of the subtraction imaging to the dynamic MRI (P < 0.001) with moderate degree of agreement between the 2 diagnostic tools (Kappa value = 0.491). This implies that Subtraction MRI significantly improves the reader confidence level within the assessment of treatment response following locoregional therapies for HCC.
Our findings agreed with Winters et al. [12] who reached to the identical result about the additive value of Subtraction MRI technique by removing pre-existing T1-weighted high signal from the post-processed images so the remaining high signal is solely because of enhancement which would improve reader confidence in detecting enhancement in targeted zones and thus improving the MRI assessment of the treatment response following loco-regional therapy. Subtraction MRI is reported to boost the conspicuity of enhancement in other imaging applications (Fig. 5).

A 49-years-old male patient with cirrhosis having RF ablation for right lobe focal lesion, Dynamic MRI was done with subtraction technique 1 month after RF ablation: a axial T1 showing bright signal of the ablated Lesion (yellow arrow) and hypointense signal of the ablation track (red arrow), b axial T2WI showing bright signal of the ablation lesion and track course, c axial T1WI post contrast showing bright signal of the Lesion as well as the Track, d subtraction MRI confirmed tumoral enhancement along the track course with no enhancement in the ablated lesion increased degree of confidence, in spite that e, f DWI and ADC MAP diffusion appeared restricted in both track and lesion as well
Newatia et al. [7] agreed with additive value of subtraction and located that subtraction can make subtle enhancement within a tumor more conspicuous and may remove the high T1 signal, which is usually present thanks to coagulative necrosis. It may also help differentiate the graceful, indistinct peritumoral enhancement seen in benign post treatment hyperemia from the discontinuous nodular enhancement of viable tumor (Fig. 6).

A 66-years-old male patient with cirrhosis having RF ablation for right lobe focal lesion, dynamic MRI was done with subtraction technique 1 month after RF ablation, a coronal T1WI showing bright signal of the ablated Lesion (yellow arrow) with hypointense signal of the track (red arrow), b coronal T1WI showing bright signal of the ablated Lesion, c axial dynamic T1WI Early Arterial post contrast showing bright signal of the Lesion possibly due to preexisting bright signal or due to tumoral enhancement, d axial dynamic late arterial phase the ablated site appeared inconspicuous becoming isointense to the rest of the liver parenchyma, e subtraction MRI confirmed non enhancement with well ablation of the lesion removing the native T1 signal as well as background suppression of the lesion in relation to the enhanced liver parenchyma increasing the degree of confidence
Hence, the role of added subtraction imaging being helpful for the assessment of the therapeutic efficacy for post TACE and RF Ablation for HCCs where by accomplishing this operation, any native T1 signal is removed and therefore the remaining signal on the subtracted images is merely because of enhancement. [7] (Fig. 7).

A 60-years-old male patient with cirrhosis having RF ablation for right lobe focal lesion, dynamic MRI was done with subtraction technique 1 month after RF ablation, a, b coronal and axial T1WI with the ablated focal lesion appearing heterogeneously Bright, c early post contrast thrive showing bright inconspicuous crescentic area along the medial margin of the hypointense lesion. d Delayed thrive the marginal area being isointense to the adjacent liver parenchyma; e subtraction augmented the presence of encasing crescentic lesion along the medial margin (yellow arrow) increasing the degree of confidence and accuracy. f Inspite of absence of diffusion restriction, based on subtraction findings with active tumoral residue Follow-up after 6 months revealed increase in tumor size, h T1 post contrast increased enhancing residual tumor implicating the upper and lateral margins as well (red arrow), i also confirmed by subtraction
Conclusion
Dynamic Subtraction MRI with its principal action supported digital subtraction of contrast enhanced and unenhanced T1WI sequences using an available non time consuming MRI software removing any native precontract T1 signal therefore the remnant high signal is secondary to Real Enhancement. All thermal ablative techniques produce coagulative necrosis and show almost similar imaging features on follow-up studies eliciting High T1WI signal, hence follow-up MRI assessment of the treatment response following loco-regional therapy becomes challenging. So by applying subtraction MRI; detection of enhancement areas within the high T1 signal lesions becomes more feasible increasing the degree of readers confidence and accuracy of treated lesions in follow-up Studies. So it is recommended to feature this powerful tool as a routine technique to any or all Dynamic MRI Scans of the Liver.
Availability of data and materials
All the datasets used and analysed during this study are available with the corresponding author on reasonable request.
Abbreviations
- HCC:
-
Hepato-cellular carcinoma
- min:
-
Minute
- mm:
-
Milli meter
- mm2 :
-
Milli meter squared
- mmol:
-
Milli mole
- MRI:
-
Magnetic resonance imaging
- msec:
-
Milli second
- RFA:
-
Radio-frequency ablation
- SPSS:
-
Statistical package for the social sciences
- TE:
-
Time to echo
References
Abdallah MFH, Desouky SHI, Madbouly M, Hassan M, Hanna A, Mahmoud AA, Abdelmaksoud MHHK (2021) Follow-up after radiofrequency ablation of hepatocellular carcinoma; diffusion weighted and dynamic contrast enhanced MRI characteristics. Med J Cairo Univ 89(1):297–305
Lee DH, Lee JM, Lee JY, Kim SH, Yoon JH, Kim YJ, Han JK, Choi BI (2014) Radiofrequency ablation of hepatocellular carcinoma as first-line treatment: long-term results and prognostic factors in 162 patients with cirrhosis. Radiology 270:900–909
Özkavukcu E, Haliloglu N, Erden A (2009) Post-treatment MRI findings of hepatocellular carcinoma. Diagn Interv Radiol 15:111–120
Kamel IR, Morgan HR (2011) MRI appearance of treated liver lesions. In: Proceedings of the international society for magnetic resonance in medicine, vol 19
Kim KW, Lee JM, Choi BI (2011) Assessment of the treatment response of HCC. Abdom Imaging 36:300–314
Kierans S, Elazzazi M, Braga L (2010) Thermoablative treatments for malignant liver lesions: 10-year experience of mri appearances of treatment response. AJR 194:523–529
Newatia A, Khatri G, Friedman B (2007) Subtraction imaging: applications for nonvascular abdominal MRI. AJR 188:1018–1025
Mahmoud BEMH, Fatooh S, Abdelmaksoud AHK (2015) Cairo/EG, C-0112, ECR
Kierans AS, Elazzazi M, Braga L, Leonardou P, Gerber DA, Burke C, Qureshi W, Kanematsu M, Semelka RC (2010) Hermoablative treatments for malignant liver lesions: 10-year experience of mri appearances of treatment response. Am J Roentgenol 194:523–529. https://doi.org/10.2214/AJR.09.2621
Hussein RS, Tantawy W, Abbas YA (2019) MRI assessment of hepatocellular carcinoma after locoregional therapy. Insights Imaging 10:8. https://doi.org/10.1186/s13244-019-0690-1
Granata V, Petrillo M, Fusco R, Vananzio S, Castleguidone EL, Catalano O, Piccirillo M, Petrillo A, Izzo F, Albino V (2013) Surveillance of HCC patients after liver RFA: role of RI with hepatospecific contrast versus three-phase CT scan 2013 gastroenterology research and practice, vol 2013, Article ID 469097, 9
Winters SD, Jackson S, Armstrong GA et al (2012) Value of subtraction MRI in assessing treatment response following image-guided loco-regional therapies for hepatocellular carcinoma. Clin Radiol 67:649–655
Morsi HA, Refaat MM, Galal OT (2020) The role of diffusion weighted MRI in the assessment of post ablation HCC viability. BMFJ 37(2):326–339. https://doi.org/10.21608/bmfj.2020.15390.1028
Acknowledgements
Not applicable.
Author information
Authors and Affiliations
Contributions
HE, MF, WM and MI, and contributed equally to this work. HE and WM designed research. WM and MF performed research. HE and MF analyzed data. HE and MI wrote the paper. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study way approved by the research ethics committee of the Private Radiology center it was applied in. No reference number available.All patients included in this study gave a written informed consent to participate in the research. If the patient was less than 16 years old, or unconscious at the time of study, written informed consent was given by their parent or legal guardian.
Consent for publication
All patients included in this study gave a written informed consent to publish the data contained in this study. If the patient was less than 16 years old, or unconscious at the time of study, written informed consent was given by their parent or legal guardian.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El-Assaly, H., Abdallah, M.F.H., Mohamed, W.M. et al. Additive role of dynamic subtraction MRI in assessment of unresolved HCC post-radiofrequency ablation. Egypt J Radiol Nucl Med 52, 257 (2021). https://doi.org/10.1186/s43055-021-00636-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-021-00636-5