- Research
- Open access
- Published:
Assessment of low-cost surgical metallic clip placement for tumor localization in BIRDAS VI breast cancer patients undergoing neoadjuvant chemotherapy
Egyptian Journal of Radiology and Nuclear Medicine volume 53, Article number: 71 (2022)
Abstract
Background
Neoadjunvant chemotherapy has become a challenging connotation for both surgeons and radiologists due to the high clinical response up to dramatic pathological complete response (pCR) that may hinder proper localization of any residual tumoral tissue. So the radiopaque markers implantation at the tumor bed became a reliable and recommended method for tumor localization before surgical intervention or NAC. Many types of commercial clips and markers are available; however they are relatively of high cost and represent a considerable burden on the governments and the heath institute that made the researchers study cheaper alternatives as standard titanium based cholecystectomy surgical clips for tumor localization.
Results
The study was conducted on 45 patients where 57 clips were inserted corresponding to number of lesions found in the total number of the patients. The response to Neoadjunvant chemotherapy was recorded and showed that 6 patients (about 13.3%) had complete radiological response after NAC, while 27 patients (60%) had regressive course after the treatment. The low cost surgical clips were evaluated by using sono-mammography and magnetic resonance imaging, and complications that occurred were recorded. Our study showed that in only 2 patients (3.5%) there was difficulty in clip visualization by Ultrasound during post-treatment follow up. In 45 patients, all the inserted clips (100%) were well visualized as small signal void on MRI at both T1WIs and T2WIs sequences, and the primary malignancy was easily visualized on both MRI and sono-mammography not interfering with the image interpretation and judgment. As regards the reported complications, our results revealed that in only 2 patients (3.5%) there was evidence of positive clip migration, while only 2 patients (3.5%) developed hematoma during the procedure as shown by ultrasound, Also 4 patients (7%) complained of pain only shortly after clip insertion. No other significant complications like infection or heat sensation developed either during the procedure or during MRI. The total price of the surgical clips was calculated with average cost of the needle about 10 US$ equivalent to 170 LE Egyptian pounds and the clip about 1.3 US$ or 20 Egyptian pounds, which is considered of lower cost when compared to the commercial breast markers of different companies with an estimated price range for clip = 75–200 US$ (average 90 US$). So insertion of surgical clips saved about 1135 Egyptian pounds equivalent to 73–75 US$ per clip placement.
Conclusion
We concluded from our study that the use of breast markers are mandatory before NAC where Surgical clips can safely substitute the commercial tissue markers as tumor localizers as they are effective, safe, well tolerated, easily visualized on imaging and do not interfere with assessment of the treatment response, with no evidence of complications and are of low cost compared with the commercial breast clips.
Background
Breast malignancy is one of commonest tumor affecting women, representing 31% of overall tumors affecting the female population. Also, 10% of the females have the risk of developing breast cancer at some stage in their life [1], The rate of breast cancer in women is increasing each year while the age at initial diagnosis is shifting to a younger age and the increase in breast cancer incidence is accompanied by an increase in the clinician and researchers concerns in the improvement of diagnostic and therapeutic tools [2].
The treatment options determining the therapeutic choice in primary breast cancer patients are becoming variable. And new therapies are now added to the usual chemotherapy regimens resulting in dramatic change in the treatment strategies of breast cancer over the past decade [3].
Neoadjuvant chemotherapy (NAC) is now considered the standard of care for breast cancer patients with operable or inoperable tumors [1], the values of NAC appeared in decreasing the mortality incidence, changing the surgical approach as the use of breast conservative surgery (BCS) and converting the inoperable lesions into operable ones. It also assisted in early detection of tumor response to therapy and tumor biology of breast cancers [4].
Multiple studies demonstrated high clinical response rate to the NAC with success rates reaching to about 80–90%. The response of breast cancer to NAC assessed using pathologic complete remission (pCR) and in some patients complete clinical, radiological and pathological response can be attained following NAC [2], this dramatic pCR may hinder proper localization of any residual tissue by the radiologists or the surgeon [1].
If complete tumor response can be achieved, accurate and reliable detection of the tumor bed after NACT by radiology and pathology is required. The use of radiodense marker clips has been shown to be an effective and reliable method to identify the region of interest. The clip can be detected by either ultrasound or mammography, and wire marking of the already inserted clip can be performed to guide the surgeon to the tumor bed [2].
For this reason, the international breast cancer specialist panel in 2006 and 2010 announces the importance of radiopaque marker localization into the breast cancer before the start of NAC or before surgical resection (even reconstructive surgery) in patients who received NAC [2].
Application of breast markers adds more progress in the field of interventional radiology in concerns with breast cancer as such clips are inserted using the ultrasound-guided technique [5].
Although there are many types of commercial clips and markers: however, they are relatively expensive and represent quite a considerable economic burden that encourages the researchers to search for other lower cost alternatives such as titanium cholecystectomy surgical clips [5]. Titanium-based metallic clip markers are used in many parts of the world for tumor localization and they are placed within the tumor under image guidance either mammography or sonography [2].
Aim of the study
Our study aimed to investigate the feasibility and cost effectiveness of using sonographically-guided indigenous low-cost surgical clips as tumor localization markers by sonomamography and Magnetic resonance imaging, this including their complications and influence on the imaging assessment after NAC.
Patients and methods
A prospective study conducted on patients who were referred to the Radiology Department, with pathologically proved malignant breast lesion/s for clip insertion.
Inclusion criteria:
-
All adult Female patients with histopathologically proven breast carcinoma (BIRADS VI) who were scheduled to undergo NAC with early stage disease were included (up to stage II).
Exclusion criteria:
-
Patients with locally advanced breast cancer or stage IV disease will be excluded.
-
Patients with a high bleeding profile or patients with no available histopathological data for the breast lesions will be excluded from the study (Fig. 1).
-
Patients with contraindications to intravenous MRI contrast administration, e.g.: allergic to IV contrast, high serum creatinine, low GFR or severe renal impairment.
-
Patients with contraindications to MRI as: claustrophobic patients, high grades of obesity may not be fit with certain MRI machines, pace makers or metallic artifact.
-
Recurrent cases and pregnant females.

Histopathology distribution of the breast lesions among study group
Ultrasound guided clip insertion was done using disposable Guillotine biopsy needle 14 G × 20 cm GTA®, with continuous real-time scanning during needle placement (Fig. 2). The needle stylet is removed and fit single GRENA® surgical titanium ligation clip into the bore of the needle transducer. The coaxial needle was advanced along the anesthetized track. Attempts should be made to identify the needle as soon as it enters the breast. It is imperative to know where the tip of the needle is at all times, thereby precluding the possibility of inadvertent puncture of an unintended structure (i.e., the chest wall). If the transducer and the needle maintain the same longitudinal axis, complete needle visualization is ensured. The stylet was used to deploy the 2–4 mm titanium clip into the center of the lesion followed by removal of the biopsy needle with the stylet. The clip is inserted in the center of the lesion and if there were the multiple or large breast cancers, additional clips were placed for lesion extent bracketing as per the radiologist’s judgment. Then sono-mammography was done immediately after clip insertion for confirmation of the site of the clips and exclusion of any immediate complications, and after that the patients started neoadjunvant chemotherapy regimen.

Schematic diagram of the preoperative ultrasonography (US) guided surgical clip insertion. A The coaxial guiding needle with an inner stylet and surgical clips. B Under US-guidance (blue), the coaxial guiding needle (white) is inserted into the center of the breast cancer (pink), and one or two clips (black) are passed through. The inner stylet (light blue) is reinserted for pushing the clip (Quoted from Young et al. [1])
Breast magnetic resonance examinations was performed at the start of the Neoadjunvant chemotherapy, using a 1.5 T machine (Achieva and Ingenia, Philips medical system, Eindhoven, Netherlands) using phased array breast coil with IV gadolinium injection with a dose of 0.1 mmol/kg (or 0.2 mL/kg) and a flow rate of 1–2 mL/s flushed by 20 mL of physiological saline. Slice thickness was less than or equal to 3 mm with pixel size less than 1 mm on each side. Acquisition time was less than 2 min as the mean enhancement time of a malignant tumour is between 90 and 120 s. Morphological sequences was taken as follows: T2W-TSE (AXIAL), T1W-TSE (AXIAL), STIR sequences (AXIAL), Dynamic T1-weighted gradient echo after IV gadolinium injection, T1W-TSE + C, SAG-LT + C SENCE, SAG-RT + C SENCE, COR + C SENCE, Diffusion-weighted imaging (DWI SSh) and ADC.
Images acquired were evaluated for the following parameters: lesion morphology and extension, the degree of artifact exerted by the clips and its effect on characterization of the lesion and location of clip.
The initial and follow up by sono-mammography after finishing the NAC was performed by Logic P9 ultrasound machine (GE—General Electric Healthcare—USA) with a high frequency linear array transducer 8–15 MHz and senographe pristina, GE healthcare mammography machine with the mean time interval between the insertion of the clip to preoperative follow up sonomammography was about 24 weeks ± 2 weeks (about 6 months or after about 8 sessions of NAC). The follow up sonomammography was assessed for: location of the clips and exclusion of any complications as clip migration by comparing the distance of the clip to the last sonomamography done before NAC on three coordinate points on mammography film (distance from the nipple, from the skin and from the muscle), displacement was recorded if there was > 1 cm difference in the clip position, and finally the effect of the clip on the image interpretation and the assessment of response to treatment according to RECIST criteria (Response evaluation criteria in solid tumors) (Tables 1, 2).
Patients with lesions no more palpable by the surgeons after the treatment were referred back to the Intervention radiology department for pre-operative wire localization over the already placed clips.
Cost-effectiveness was determined by calculating the cost of the surgical clips and that of the commercial metallic markers, while cost saving was calculated by comparing the two values.
Statistical analysis
Recorded data were analyzed using the statistical package for social sciences, version 20.0 (SPSS Inc., Chicago, Illinois, USA). Quantitative data were expressed as mean ± standard deviation (SD). Qualitative data were expressed as frequency and percentage.
The following tests were done:
-
Chi-square (× 2) test of significance was used in order to compare proportions between qualitative parameters.
-
The confidence interval was set to 95% and the margin of error accepted was set to 5%. So, the P value was considered significant as the following:
-
Probability (P value)
-
P value < 0.05 was considered significant.
-
P value < 0.001 was considered as highly significant.
-
P value > 0.05 was considered insignificant.
-
Results
The study was conducted on 45 patients with a wide age group ranging from 28 to 64 years, (mean age of 46.42 ± 9.87 years), with total number of inserted clips were 57 corresponding to number of lesions found in the total number of the patients.
Our results showed that 6 patients (about 13.3%) had complete radiological response after NAC; in addition 27 patients (60%) had regressive response after the treatment (Table 3).
As regards sonomamographgic assessment of breast clips, In 55 lesions (96.5%) the clip was easily visualized as linear hyperechoic structure compared to 2 lesions (3.5%) showed difficulty in clip visualization by ultrasound during the follow up study after the treatment. Also our results showed that in 18 lesions (31.6%) there was clip artifact with posterior acoustic shadowing, yet not interfering with images interpretation or assessment of the treatment response.
As regards MRI, the results showed that in 45 patients (100%) all the surgical clips created a small signal void on MRI which was more appreciated at both T1WIs and T2WIs sequences, however, the primary malignancy was easily visualized on MRI and not affecting with the image interpretation and judgment as regards the characterization of the lesion or the pattern of enhancement (Fig. 3).

MRI clip assessment distribution among study group
As regards the complications, in only 2 patients (3.5%) there was evidence of positive clip migration during the preoperative follow up yet not interfering with the judgment upon the tumor assessment and response to NAC. Only 2 patients (3.5%) were complicated with hematoma immediately during the procedure as shown by ultrasound, Also 4 patients (7%) complained of Pain only shortly after the procedure (Fig. 4).

Complications of clips insertion distribution among study group
The study was conducted on a wide cost of surgical clips for each patient ranging from 10 to 32 US$ equivalent to 170 to 510 Egyptian Pounds, (mean cost of 13.89 ± 6.777 US$ equivalent to 215.33 ± 105.05 Egyptian Pounds), with the average cost of the needle = 10 US$ (170 LE Egyptian pounds) and the clip = 1.3 US$ (20 Egyptian pounds). When compared to the commercial breast markers with an estimated price range for clip = 75–200 US$ (average 90 US$). So application of surgical clips saved about 1135 Egyptian pounds equivalent to 73–75 US$ per clip (Fig. 5).

Cost of surgical clips (LE) among study group
Discussion
-
The study that we carried stands out the potential role of using low cost titanium surgical metallic clips for tumor localization in patients planned for neoadjunvant chemotherapy (NAC) before surgical treatment.
-
Breast cancer is disease with heterogeneous etiology associated with different characteristic histological and biological features, clinical presentations, and therapeutic responses. The most common type of breast carcinoma is the so called invasive ductal carcinomas [6]. That was in agreement with our results that showed the most frequent pathological type of breast cancer seen among the studied group was IDC grade I, followed by IDC grade II and last IDC grade III (Figs. 6, 7).
Fig. 6 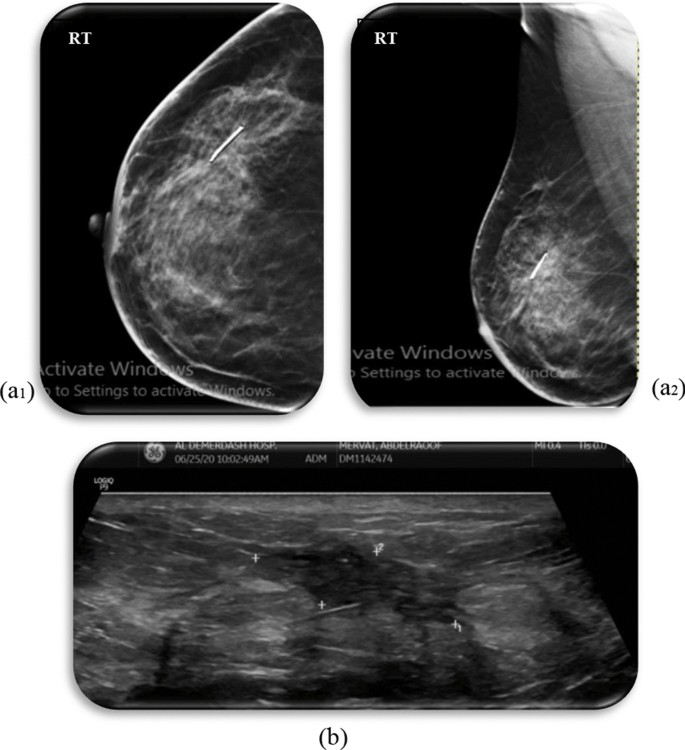
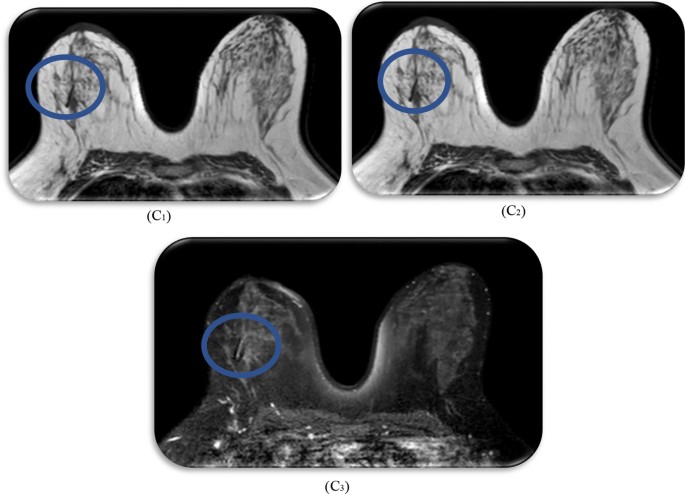
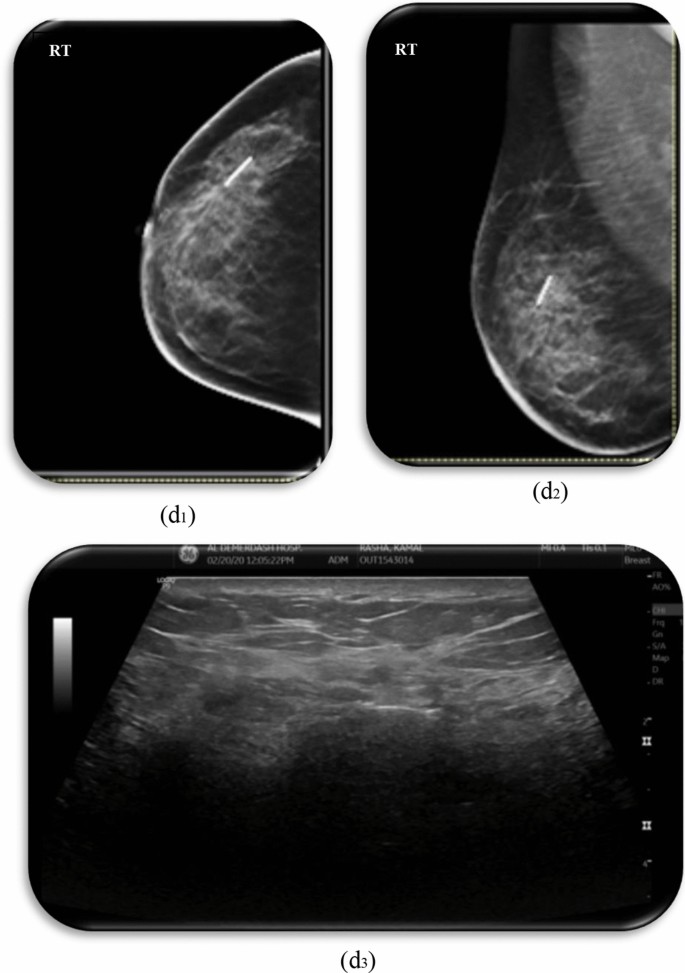
40-year-old patient with recently pathologically proven invasive ductal carcinoma (IDC) grade II, planned for neoadjuvant chemotherapy came for metallic clip placement. Breast sonomamgraphy after clip placement a1 CC View, a2 MLO view and b ultrasound images showing the surgical clip seen within the upper outer quadrant mass lesion with no significant clip artifact interfering with the image interpretation or evidence of instant complications. MRI both breasts c1 T1WIs, c2 T2WIs and c3 post contrast images done after one month of clip insertion and after start of neoadjunvant chemotherapy showing small signal void due to the clip observed in the center of the proven malignant lesion yet there was no difficulty in characterization of the lesion. After completing the course of neoadjuvant therapy, follow up sonomamography was done d1 CC views, d2 MLO view and d3 ultrasound images showing the regressive course as regards the right side upper outer breast lesion where the surgical clips are seen at the lateral end of the remaining lesion as seen on the ultrasound images where the clip seen in-place on sonomamography images which proves to be a pseudo-displacement
Fig. 7 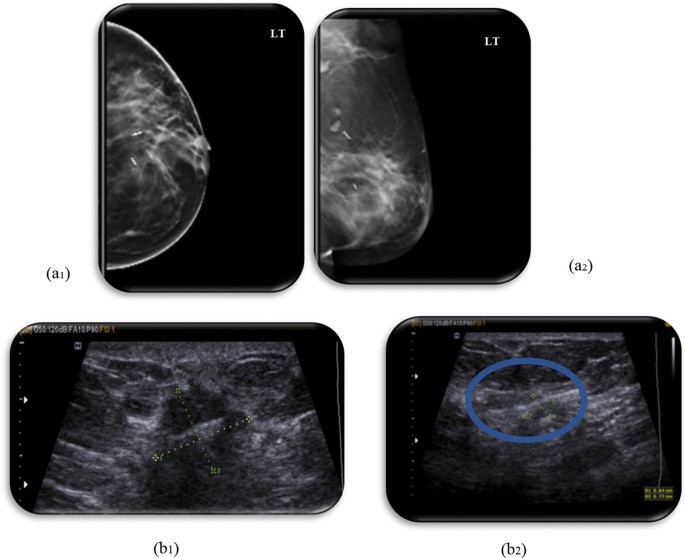
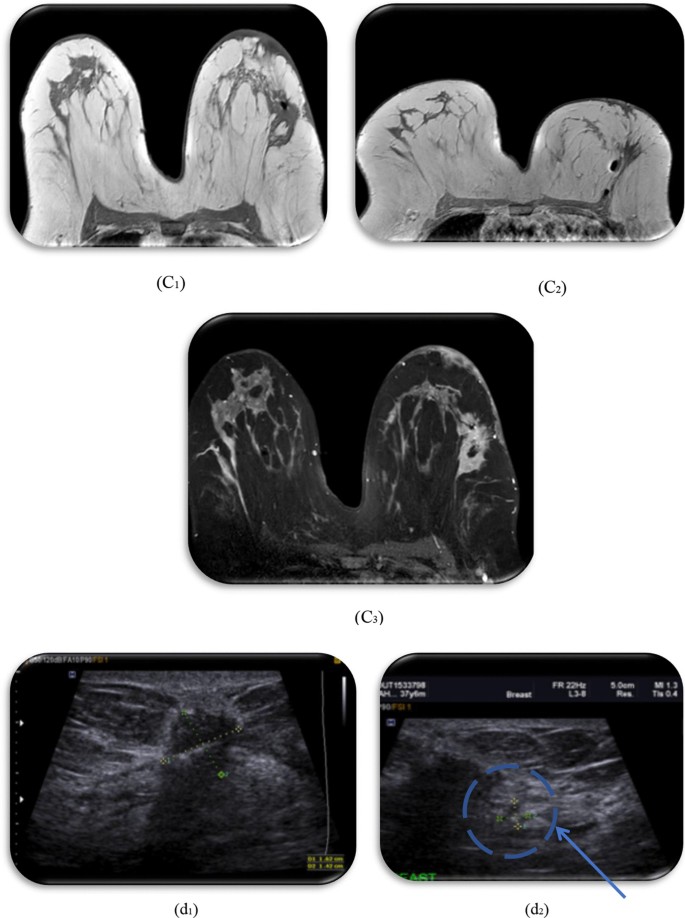
37-year-old patient with left breast lump, recently pathologically proven invasive ductal carcinoma (IDC) grade II came for clip insertion before the start of chemotherapy, Breast sonomamography after clip placement a1 CC view, a2 MLO view and b1 ultrasound images showing the surgical clip seen within the left breast lobulated hypoechoic mass (b2) with an adjacent smaller satellite lesion with a clip seen inside, yet both clips show no artifact interfering with images interpretation. MRI of both breasts c1 T1WIs first clip inside lesion c2 T1WIs second clip and c3 post contrast) done showing a signal void of two metallic surgical clips seen at UOQ, still seen inside two left sided ill-defined speculated malignant mass lesions showing evidence of post contrast enhancement. After completing the course of neoadjuvant therapy, follow up sonomamography was done d1 and d2 shows two surgical clips still noted in left breast solid masses showing regressive course as regards the size with the clips still seen in the same site compared to the previous studies
-
NAC is considered a cornerstone step in the treatment of breast carcinoma especially in its early stages, as it results in decreasing the mortality incidence, changing the surgical approach with better surgical outcomes by conserving the breast by breast conservative surgery (BCS) or lumpectomy instead of for example modified radical mastectomy (MRM), convert the inoperable lesions into operable ones, lessening the unfavorable postoperative complications and improving cosmetic outcomes [7]. It also assists in early detection of tumour response to therapy and tumour biology of breast cancers [4].
-
In one systematic review of neoadjuvant chemotherapy for operable breast cancer, patients receiving neoadjuvant chemotherapy had a lower mastectomy rate than those undergoing surgery before adjuvant chemotherapy [8].
-
The National Cancer Comprehensive Network guidelines recommend clip insertion before NAC, as the radiologists cannot predict the exact outcome of NAC which may be adequate enough up to complete radiological response associated with difficult identification of the tumor site by the surgeon during surgery.
-
As NAC has become more common, breast markers become more essential as it help in identification of tumor bed especially with cases with complete radiological response. Markers can be removed with the cancerous lesion or left in place after surgery without serious complications [9].
-
In Our study, we tried to use the surgical clips as substitute of the commercial breast markers aiming to reduce the cost of this procedure. There have been many types of commercial breast markers launched by different companies. Lobbes et al. [4], found that cheaper surgical clips be made of safe materials as titanium, have been approved by the KFDA (Korea Food & Drug Administration).
-
In Our study, the surgical clips were inserted by needle used in the Core breast biopsy (Core needle biopsy CNB) by US-guided automated technique using a commercial coaxial guiding needle. This was in agreement with Hassan et al. [2], who used disposable Guillotine biopsy needle 16G x 20 cm GTA® with the similar automated technique that is similar to the core breast biopsy technique that is considered a safe easy procedure done completely under real-time ultrasound surveillance to identify the desired location for the surgical clips with an estimated time of the whole procedure about 6–10 min.
-
The surgical breast marker can be placed at the (CNB) performed site where there is no tissue injury due to repeated insertion and less bleeding with lower probability of tumor cell seeding. Kaufmann et al. [9], found that on performing on-site clipping immediately after CNB both the medical costs and procedure time can be lower than those of the two-step clipping procedure.
-
US-guided CNB technique is performed with real-time imaging surveillance which is considered as a relatively safe method with few reported complications or adverse events. Therefore, the insertion process itself is not considered an onerous duty by breast radiologists [1].
-
Our study was based on the hypothesis that radiopaque markers can replace commercial breast markers for tumor localization as well as for the assessment of tumor response after NAC, yet without interfering with radiologic multimodality evaluation including sono-mammography and MRI, with no significant complications and with lower cost. That what was illustrated as follows.
-
As regards the complications of the clip; the migration of surgical clips and related complications can be a limitation of surgical clip insertion. Clip migration may occur immediately after biopsy or may be seen on later follow-up sono-mammograms [1].
-
In our study only 2 patients (3.5%) showed radiological evidence of clip displacement where there were > 1 cm difference between the distance of the clip at the pretreatment sonomamography and follow up sono-mammography after NAC, yet not interfering with image interpretation. Those results were close to Hassan et al. [2] study, who used US guided inserted surgical clips followed by follow up sono-mammography after treatment, and reported two cases representing about 6.25% with positive clip migration.
-
In our study, from the cases that showed regressive course regarding the size of the lesion, two cases had evidence of clip displacement. In those two cases there was no change in the clip distance measured at the mammography images on three different quadrants (distance from skin, from areola and from chest wall), only the displacement was noted on ultrasound images, which confirms that the clip did not move, but the primary lesion changed in size in relation to the clip.
-
That was explained by Lee et al. [10] who found that the cause of clip migration is the change of the size and shape of the tumor in which the clip was deployed after NAC or radiotherapy, which may be misinterpreted as clip migration.
-
Our result wasn't in agreement with Hassan et al. [2], and Margolin et al. [11] who explained the cause of the clip migration due to predominant fatty elements of the breast tissue ACR (a) which may cause redundant breast tissue and low tissue resistance. But the point of disagreement was that the two cases in our study with positive migration had a heterogeneous breast tissue categorized as ACR (c), which couldn’t explain the cause of displacement in our study.
-
There are different breast cancer types, but the most common type of breast carcinoma is so called invasive ductal carcinomas and in most of the cases breast cancer appears as solid irregular or speculated lesions with some lesions may show areas of cystic degeneration or necrosis. The variations in breast density, tumor composition as solid with or without or cystic degeneration or necrosis and consequently the tissue resistance was seen to be a factor affecting the degree of clip migration. The low tissue resistance as in fatty breasts may allow clips to easily migrate by interfering with the fixation of surgical clips especially after decrease in the size of the mass which is an important factor for clip fixation and stability.
-
Previous studies on clip migration as Hassan et al. [2], and Margolin et al. [11] have shown that clips move more easily in fatty breast tissue; however, Carolyn et al. [12] showed that some of this apparent migration may be also due to the greater pliability and mobility of the fatty breast. However, clips are generally inserted into the center of the mass or the most solid component with higher tissue resistance because of its solid nature. Thus, the chance of clip migration should be lower.
-
Results also shows that, there were only 2 patients (about 3.5%) had hematoma during the procedure as shown by ultrasound, and only 4 patients (7%) complained of pain shortly after the procedure.
-
Our results revealed that the rest of the patients had no evidence of pain or heat sensation either during the procedure or during MRI, also the rest of the study population showed no evidence of hematoma formation or infection. All the above data confirms that the clip insertion is highly significant complication-free procedure, that was agreed with Young et al. [1], who showed no significant complications along the studied group
-
As regards sono-mammographgic assessment of the clip, our study shows that: from the total number of inserted clips, 55 clips (96.5%) were easily visualized as linear hyperechoic structures compared to 2 clips (3.5%) showed difficulty in visualization by Ultrasound that was noted during the follow up after receiving NAC. These results were in-agreement with Young et al. [1] who found 100% of the inserted clips appeared as linear hyperechoic structures on the ultrasound.
-
That also stands with Koo et al. [13], who compared between the surgical clips and commercial breast markers found that marker visibility was little more common when using Liga Clip (surgical clips) (about 91.1%, 51 of 56) than when using Cormark markers (commercial clips) (about 86.9%, 53 of 61) in all cases. And in cases where no residual lesion could be noted on US during the follow up after NAC, marker visibility was more common when using LigaClip markers (88.2%, 15 of 17) than when using Cormark markers (80% 8 of 10).
-
The two cases in which there was difficulty in clip visualization showed complete radiological response. Won et al. [14] explained the previous findings on the hypothesis that the hyperechoic (metallic) clip can be easily visible against the background of the hypoechoic nature of the tumor. When the tumors becomes smaller and even disappear as NAC proceeds this hinders differentiating the clip from the background of the echogenic fat strands.
-
Also our results showed that 18 lesions (31.6%) showed clip Artifact with posterior acoustic shadowing while 39 lesions (68.4%) showed no Clip artifact that was not in agreement with Hassan et al. [2]. study which recoded only 3 patients (9.4%) with clip artifact.
-
In our study this clip artifact did not interfere with ultrasound assessment of the lesion, where in 45 patients (100%) the clip neither interfere in assessment of the treatment response nor the morphology of the lesion by sono-mammography. That agrees with Young et al. [1], and other multiple previous studies which show that application of surgical clips even in the presence of artifact won’t interfere with neither sonographic assessment of the lesion nor the size of the lesion and therefore assessment of the treatment response.
-
As regards MRI assessment of the clip: Breast metallic clips can cause artifacts on MRI, depending on magnetic susceptibility, clip quality, size, shape, orientation, position, and used MRI parameters [1].
-
In our study, in all our patients (100%) the surgical clips created a small signal void on MRI; however, the primary lesion was easily visualized on MRI and did not interfere with the image interpretation and judgment as regards the characterization of the lesion or the enhancement pattern.
-
The inserted clips appeared on MRI as small signal voids due to its paramagnetic or susceptibility properties, which is more appreciated at both T1WIs and T2WIs, where in 15 patients (26.3%) the clips were best visualized at T1WIs, 8 patients (14%) at T2WIs compared to 34 patients (59.6%) where the clips were best visualized at both T1WIs and T2WIs images, this can be explained as T1 sequences are performed without fat saturation which allow metal markers to be better detected, this detection is based on the magnetic susceptibility artifact best seen on T1 gradient-echo sequences, created by the metallic nature of the marker. The longer the TE of the sequence the more this artifact is visible so T1 sequence was found to be best sequence for detection metallic artifact of the clip [15] (Fig. 8).
-
As regards assessment of prognosis of treatment response; the assessment of tumor response to NAC as confirmed on US, mammography, and MRI is important and done according to RECIST criteria, Response evaluation criteria in solid tumors refers to a set of published rules used to assess tumor burden in order to provide an objective assessment of response to therapy. The RECIST criteria can be used with CT, MRI or conventional radiography (in some instances) [15].
-
Tumor response to neoadjuvant chemotherapy may be either complete response (CR) with disappearance of all lesions, partial response (PR)/regressive response where > 30% decrease in sum of all target lesions in longest axis measurement, stable disease (SD) and progressive disease (PD) according to RECIST criteria [17].
-
Clearly, the ideal result for a patient undergoing neoadjuvant chemotherapy is eradication of the malignant disease in the breast and in the axillary lymph nodes (pCR).
-
In our study, there were 6 patients (about 13.3%) had radiological complete response after NAC, compared to Hassan et al. [2], study where they found 14 patients (about 43.75%) showed complete pathological response and that was close to Edeiken et al. [16] study which found 47% of the study population had complete response.
-
Also in our study there were 27 patients (60%) showed regressive course after NAC while only 10 patients (22.2%) had stationary course regarding the size of the lesions, and only 2 cases (4.4%) showed progressive disease response with highly significant difference between the studied group showing improving disease response and the other studied groups.
-
In two patients out of 27 patients who had regressive course, the lesions were not palpable by the surgeons and needed preoperative wire localization.
-
That emphasizes the role of clips insertion for localizing the site of the lesion especially in cases showing improving disease response that may interfere in radiological recognition of the site of the lesions and the tumor bed. Where in our study about 33 patients (about 73%) showed improving disease response including patients achieving a complete or near-complete response to NAC. In this situation clip insertion effectively addresses the problem of preoperative localization of the tumor and if the clip was not inserted the tumor bed, those patients could have been lost and the surgeons would have to undergo major surgical excision as Modified radical mastectomy (MRM) instead of conservative breast surgeries.
-
As regards the Cost of the clip: The study was conducted on a wide cost of surgical clips with the average cost of the needle = 10US$ equivalent to 170 LE Egyptian pounds and the single clip = 1.3 US$ equivalent to 20 Egyptian pounds with total cost per patient (170 + 20 = 190) about 190 Egyptian Pounds equivalent to 12–13 US$, compared to Hassan et al. [2], study that revealed that the average cost of the single surgical clip was 145 ± 20 LE Egyptian pounds which is almost equivalent to8–9US$. This was in agreement to Masroor et al. [17] study who found that the cost of surgical clips was about 9 US$, and similar to the study done in South Korea since 2015 where the calculated cost was 10 US$ per clip [1].
-
This is of much low cost when compared to the commercial breast markers with an estimated price range for clip = 75–200 US$ internationally (average 90 US$).
-
This means that the use of surgical clips saved about 75–76 US$ which is equivalent to 1135 Egyptian pounds that was close to Hassan et al. [2], which recorded the saved price about 80–82 US$ for each clip, this confirms that surgical clips of the highly considerable low cost compared to the commercial breast markers.







42-year-old patient with breast lump and axillary masses, the patient came for tru-cut biopsy, which shows advanced breast carcinoma, planned for neoadjuvant chemotherapy and metallic clip placement. The patient received first cycle chemotherapy and came for clip insertion, Breast sonomamography after clip placement a CC view and b ultrasound images showing the metallic clip seen inside the upper outer quadrant mass lesion with no artifact or posterior acoustic shadowing hindering proper visualization of the lesion. MRI of both breasts done after other cycle of NAC c1 T1WIs, c2 T2WIs, c3 post contrast images and c4 subtracted post contrast images) showing the signal void of the inserted surgical clip inside the previously noted breast lesion, with no difficulty in characterization of the lesion. After completing the course of neoadjuvant therapy, follow up sonomamography was done d1 ultrasound image and d2 MLO view showing the surgical clips still seen at the left breast irregular mass lesion which shows appreciable regressive course as regards the size with the clip still seen in the same site compared to the previous studies e ultrasound image shows preoperative wire localization guided by the previously inserted surgical clip due to appreciable regressive course of the size of the lesion
Conclusion
Our study proved that the use of breast markers is mandatory before NAC where sonographically-guided metallic surgical clips can safely substitute the commercial tissue markers as tumor localization. Surgical clips are effective, considerable and safe for the patient, easily visualized on imaging, do not interfere with assessment of treatment response, with no evidence of complications and are of low cost compared with the commercial breast clips.
Limitations
-
In our study group, The most common type of breast carcinoma was invasive ductal carcinomas, with most of the lesions were solid and no complex cystic lesions nor any cystic degeneration were detected, which made us unable to precisely study the effect of the tissue resistance and nature on the radiological assessment of the clip and detection rate of clip migration.
-
Relatively small sample size, and that was due to high cost of MRI and presence of some contraindication in some patients.
Recommendations
-
For further multi-parametric studies, we recommend applying the one step clipping procedure and to place the surgical clip at the same setting of the core tissue biopsy to avoid repeating insertion of the needle, minimize tissue injury, decrease incidence of tumor cell seedling and to lower the cost and the procedure time.
-
Also, other studies are needed to study this technique over larger number of patients to detect the rate clip migration on other lesions with different histological types and different tissue natures.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- NAC:
-
Neoadjuvant chemotherapy
- MRI:
-
Magnetic resonance imaging.
- pCR:
-
Pathological complete response
- rCR:
-
Radiological complete response
- GFR:
-
Glomerular filtration rate
- CNB:
-
Core needle biopsy
- RECIST:
-
Response evaluation criteria in solid tumors
References
Young IY, Seon HC, Shin HK et al (2015) Ultrasonography-guided surgical clip placement for tumor localization in patients undergoing neoadjuvant chemotherapy for breast cancer. J Breast Cancer 18(1):44–49. https://doi.org/10.4048/jbc.2015.18.1.44
Hassan SA, Osman MA (2018) Cost-effectiveness of ultrasound-guided surgical clips placement for breast cancer localization prior to neoadjuvant chemotherapy. Egypt J Radiol Nucl Med 49:1163–1168
Vander WA, Hurria A (2012) Early breast cancer in the older woman. Clin Geriatr Med 28:73–91
Lobbes MB, Prevos R, Smidt M et al (2013) (2013) The role of magnetic resonance imaging in assessing residual disease and pathologic complete response in breast cancer patients receiving neoadjuvant chemotherapy: a systematic review. Insights Imaging 4:163–175
Le-Petross HC, Hylton N (2010) Role of breast MR imaging in neoadjuvant chemotherapy. Magn Res Imaging Clin North Am 18(2):249–258
Ellis P, Schnitt SJ, Sastre-Garau X et al (2003) Invasive breast carcinoma. In: Tavassoli FA, Devilee P (eds) WHO classification of tumours pathology and genetics of tumours of the breast and female genital organs. IARC Press
Kim Z, Min SY, Yoon CS, Lee HJ et al (2014) The basic facts of Korean breast cancer in 2011: results of a nationwide survey and breast cancer registry database. J Breast Cancer 17:99–106
Mieog JSD, van der Hage J, van de Velde CJH (2007) Neoadjuvant chemotherapy for opérable breast cancer. Br J Surg 94:1198–1200
Kaufmann M, von Minckwitz G, Mamounas EP et al (2012) Recommendations from an international consensus conference on the current status and future of neoadjuvant systemic therapy in primary breast cancer. Ann Surg Oncol 19(1508–16):8
Lee SG, Piccoli CW, Hughes JS (2001) Displacement of microcalcifications during stereotactic 11-gaugedirectional vacuum-assisted biopsy with marking clip placement: case report. Radiology 219(495–497):10
Margolin FR, Kaufman L, Denny SR et al (2003) Metallic marker placement after stereotactic core biopsy of breast calcifications: comparison of two clips and deployment techniques. Am J Roentgenol 181:1685–1690
Carolyn RM, Meredith AK, Chris JDM et al (2015) Radiographer technique: does it contribute to the question of clip migration? J Med Imaging Radiat Oncol 59:564–570
Koo JH, Eun-Kyung K, Hee JM, Jung HY, Vivian YP, Min JK (2019) Comparison of breast tissue markers for tumor localization in breast cancer patients undergoing neoadjuvant chemotherapy. Ultrasonography 38(4):336–344. https://doi.org/10.14366/usg.19004
Hk W, Hye JK, See HK et al (2019) Ultrasound-guided dual-localization for axillary nodes before and after neoadjuvant chemotherapy with clip and activated charcoal in breast cancer patients: a feasibility study. BMC Cancer 19:859. https://doi.org/10.1186/s12885-019-6095-1
Orlacchio A, Bolacchi F, Rotili A et al (2008) MR breast imaging: a comparative analysis of conventional and parallel imaging acquisition. Radiol Med 113:465–476
Edeiken BS, Fornage BD, Bedi DG et al (1999) US-guided implantation of metallic markers for permanent localization of the tumor bed in patients with breast cancer who undergo preoperative chemotherapy. Radiology 213:895–900
Masroor I, Zeeshan S, Afzal S et al (2016) Outcome and cost-effectiveness of ultrasonographically guided surgical clip placement for tumor localization in patients undergoing neoadjuvant chemotherapy for breast cancer. Asian Pac J Cancer Prev 16(18):8339–8343
Acknowledgements
The author thanks all the study participants for their patience and support.
Funding
This study had no funding from any resource.
Author information
Authors and Affiliations
Contributions
NOS: collected and analyzed the data, wrote the manuscript, prepared the cases, performed required interval procedure, measurements and statistical analysis, and prepared figures and tables. SFI: suggested the research idea, shared in data collection and analysis, reviewed literature, statistical analysis, and manuscript editing. AIH: reviewed the manuscript and statistical analysis. RHA: reviewed the manuscript and statistical analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Research Ethics Committee of the Faculty of Medicine at Ain Shams University in Egypt in March 2020; Reference number of approval: MD87/2020.
Consent for publication
All patients included in this research gave written informed consent to publish the data contained within this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Abdelfatah, N.O.S., Abdallah, R.H., Ibrahim, S.F. et al. Assessment of low-cost surgical metallic clip placement for tumor localization in BIRDAS VI breast cancer patients undergoing neoadjuvant chemotherapy. Egypt J Radiol Nucl Med 53, 71 (2022). https://doi.org/10.1186/s43055-022-00740-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00740-0