- Research
- Open access
- Published:
Role of MR enterography versus ileo-colonoscopy in the assessment of inflammatory bowel diseases
Egyptian Journal of Radiology and Nuclear Medicine volume 54, Article number: 17 (2023)
Abstract
Background
Inflammatory bowel disease (IBD) is widespread and rapidly rising in developing countries. It remains a significant issue in Western culture with a prevalence of more than 0.3%. Symptom control has been the only focus of treatment before the discovery that many individuals with IBD continue to have disease activity even in the absence of clinical symptoms. Therefore, treatment goals now include establishing clinical remission, steroid-free remission, and mucosal healing, which may eventually be complemented by transmural healing in cross-sectional imaging modalities. Magnetic resonance enterography (MRE), computed tomography enterography, and small-bowel ultrasound are now reliable methods for staging intramural lesions and extramural consequences in CD and for determining disease activity and severity. Recently literature suggests the incorporation of (MRE) for periodic reevaluation of IBD patients, as it offers small-bowel, colonic, and extra-enteric assessment as well as monitors the response to the anti-inflammatory therapy. The purpose of the current study was to compare MRE with ileo-colonoscopy findings in the diagnosis of IBD features, specifically Crohn's disease, and ulcerative colitis, as well as in the detection of disease exacerbation (Activity).
Results
This study used MRE and ileo-colonoscopy to assess chronic inflammatory bowel disease patients; the patient population (n = 30) was made up of (14/30, 46.7%) females and (16/30, 53.3%) males, with a mean age of 32 ± SD 13 years. MRE alone detected lymphadenopathy in 73.3% of patients, and mural thickening with a mean of 4.1 ± SD 5.1 mm. It has detected mucosal enhancement with 80% sensitivity and 60% specificity. However, it was unable to detect mucosal erosions or ulceration.
Conclusions
MRE is sensitive, inexpensive, noninvasive, and radiation-free for inflammatory bowel disease detection, with 86.7% diagnostic accuracy for affected areas. Unlike ileo-colonoscopy, it could examine the entire small intestine, precisely measure the affected loop, and detect activity signs such as mural thickening and lymphadenopathy. Only ileo-colonoscopy could detect mucosal degradation and superficial ulcers. IBD treatment protocols should incorporate MRE for small-bowel, colonic, and extra-enteric assessment, monitoring of disease activity, and anti-inflammatory therapy response.
Background
Inflammatory bowel diseases (IBDs) are characterized by chronic idiopathic inflammation of the gastrointestinal (GI) tract. IBD patients most commonly experience Crohn's disease (CD) or ulcerative colitis (UC). Transmural inflammation, a hallmark of IBD, particularly CD, causes the GI wall to thicken and narrow, eventually resulting in the disabling development of deep lacerations, fistulae, strictures, and abscesses. Additionally, persistent deep transmural inflammation increases the likelihood of colitis-associated neoplasia and causes irreparable structural damage [1].
IBD is now a worldwide problem with a fast-increasing prevalence in poorer nations, and it is still a major problem in Western civilization, with a prevalence of above 0.3% [2].
Small-bowel imaging with magnetic resonance enterography (MRE), computed tomography enterography, and ultrasound has been shown to accurately measure disease activity and severity, as well as the staging of transmural lesions and extramural consequences in Crohn's disease (CD) [3].
Due to the failure of previous therapeutic techniques to change the course of CD, innovative treatment aims such as early intervention with effective treatment, treat to target, tight disease control, and surveillance can help patients have better results. These goals necessitate regular and timely patient assessments to track clinical (patient-reported outcomes, PRO), endoscopic (mucosal healing), and radiographic outcomes so that management can be optimized proactively [4].
Before it was realized that many individuals with IBD have ongoing disease activity even in the absence of clinical symptoms, the entire focus of treatment has always been on symptom control. Thus, instead of just treating clinical symptoms, treatment goals now include establishing clinical remission, steroid-free remission, and finally mucosal healing, which may eventually be supplemented by transmural healing in cross-sectional imaging modalities [5].
Resolution of stomach discomfort and normalization of bowel habits, as well as the absence of ulceration on ileo-colonoscopy, is the goal of the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) program in the treatment of CD. During the active period of the disease, clinical results were to be monitored every three months, whereas endoscopic outcomes were to be measured every six to nine months [1].
The rationale for this shift in treatment objectives is based on data that mucosal healing is linked to a better long-term patient outcome, as measured by a lower chance of relapse, decreased hospitalization rates, steroid-free remission in the follow-up examination, and resection-free intervals [6]. In terms of direct clinical usefulness, it has been demonstrated that individuals with CD who have mucosal healing have a lower risk of penetrating problems and surgery as compared with patients with severe ulcerations [7].
Costs, potential hazards (perforation, hemorrhage, and cardiovascular issues related to anesthesia), and lack of patient cooperation impede routine endoscopic evaluation. Nonetheless, more than two-thirds of CD patients experience inflammation of the small intestine. Unfortunately, some inflamed bowel segments may be inaccessible through endoscopy (e.g., strictures, adhesions, and proximal small bowel) [8].
MR enterography (MRE) is a sensitive imaging method that does not require ionizing radiation, which can be a significant concern in young patients with IBD. MR enterography is also useful for helping to classify newly diagnosed IBD in patients who have isolated colon disease or an indeterminate form of colitis. The detection of clinically unexpected small-bowel inflammation by MR enterography could become a crucial step in diagnosing CD and subsequently guiding therapy [9].
Endoscopy and imaging are crucial to the diagnosis and treatment of IBD. In addition to allowing the assessment of disease type and distribution, endoscopic evaluation permits the histopathological investigation required for establishing the diagnosis and separating IBD subtypes [10].
With the growing availability and experience of MRI (magnetic resonance imaging) techniques, treating physicians now have more diagnostic options for monitoring patients with CD and UC [11].
Aim of work
-
Comparison between MRE and ileo-colonoscopy findings in the detection of IBD features, and the evaluation role of MRE in the assessment of IBD patients, namely Crohn's disease and ulcerative colitis.
-
Comparison of MRE versus ileo-colonoscopy in the detection of disease exacerbation (Activity).
Methods
This study is an observational cross-sectional analytic study. Data were collected prospectively after getting ethical approval from the institutional review board (IRB) of the faculty of medicine, in our university, Code: (MS-456-2020).
Study population
The sample size was 30 adult patients who were diagnosed and on the treatment of IBD, referred from the IBD clinic, (ICRID clinic) of our institution, within the period from December 2020 to September 2021. This number was adopted by using MedCalc 19 program by setting alpha error significance of 0.05%, 95% confidence level, and 80% power sample. This study's sample size was determined by using the previous study of Alexander et al. [12] value for the Spearman correlation between the Crohn's Disease Endoscopic Index of Severity (CDEIS) and the Magnetic Resonance Index of Activity (MaRIA), which was calculated as 0.49.
Informed consent was taken from all patients before the study. The patient population (n = 30) consisted of 30 adult patients, 16 (53.3%) males and 14 (46.7%) females, with a mean age of 32 ± 13 years (range 18–81 years). This study included eligible adult males and females with evidence of IBD as diagnosed by clinical, laboratory, imaging, and endoscopic criteria. We excluded children less than 18 years, low kidney functions patients (eGFR < 30 ml/min), pregnant and lactating women as well as contraindicated patients to MRI as patients with cardiac pacemakers or claustrophobia. Besides we have excluded patients who had intervals between ileo-colonoscopy and MRE of more than 2 weeks.
Methods
Clinical and laboratory assessment
An expert gastroenterologist has documented the symptoms, physical, and laboratory findings of the patients as part of their assessment in the IBD clinic.
Endoscopic protocol
Pre-procedural oral preparation (such as laxatives, enema, and prevention of dairy products, carbonated beverages, and red-colored liquids) was used for bowel cleansing, which is essential for adequate mucosal examination. Variable types of sedation (such as propofol) with cardiac and oxygen monitoring were introduced for patient comfort, depending upon the predicted difficulty of the procedure. Bowel distention by Polyethelene Glycol was preferred for adequate mucosal examination. A full clinical examination was done, and a digital rectal examination was conducted by an expert gastroenterologist to check for skin tags, polyps, and fistulas.
A gastroenterologist with ten years of experience in colonoscopy has employed a flexible colonoscopy tube that is passed through the anus and into the colon.
A multichannel system for air insufflation, water suction, video, and power supply was attached to the colonoscope: “Olympus video-scope was used in this study,” which is supported by the magnification available with narrow-band imaging (NBI). The ileo-colonoscopy protocol is in agreement with Somwaru et al. [13]. Ileo-colonoscopy findings have represented the standard reference for the evaluation of the role of MRE.
MRI acquisition
Within 2 weeks intervals maximum after ileo-colonoscopy; patients underwent MR enterography using a 1.5 T MR scanner: “Philips Achieva 1.5 T device” using a phased array body coil. Patients were prepared before the examination with a low-residue diet for 24 h and 8 h of fasting before imaging and rectal enema before the examination procedure. Mannitol–water contrast solution was administered using 350 ml mannitol 20% over 1150 ml water. Patients were advised to start drinking one hour prior to the examination one cup (250 ml/10 min). They were asked to lie in the supine position. Three-plane localizer: from the xiphisternum to Symphysis Pubis, was done followed by the standard MR protocol for enterography in our institution as follows:
-
Axial and coronal: T2-weighted single-shot fast spin echo sequences (SSFSE) and diffusion-weighted sequences.
-
Injection of I.V. antiperistaltic agent (20 mg Buscopan) and 10 ml Magnevist I.V (0.1 mmol/kg BW), followed by dynamic coronal 3D T1-weighted gradient echo sequences with fat suppression, obtained in time intervals of 45–55, 70, and 180 s.
-
Post-contrast axial 3D T1-weighted gradient echo sequences with fat suppression is obtained between the coronal portal and delayed phases.
-
Coronal post-contrast axial 2D or 3D T1-weighted sequences with fat suppression are acquired. Coronal cuts should be at least 6 mm slice thickness and 0.5 mm gaps.
-
Our institutional protocol has been found to be in agreement with that of Yoon et al. [14].
The MRE images were interpreted by a radiologist with 12 years of experience in GIT sub-specialty, who was blinded to the ileo-colonoscopy findings.
Statistical analysis
Data were described in the form of frequencies (number of patients) and percentages using the “Microsoft Office Excel Software” application for Windows (2010).
-
Statistical analysis for the data was conducted using SPSS 22nd edition, numeric variables were presented in mean and standard deviation, and paired comparison was done using Wilcoxon sign rank test after normality testing. Categorical data were presented in frequency and percentage, and paired comparison was conducted using McNamara test. Any p value < 0.05 was considered significant.
Results
Demographic data
-
This prospective study involved thirty IBD patients who were referred from our IBD clinic. Age range 18–81 years old. The patient population (n = 30) included 16 (53.3%) males and 14 (46.7%) females with a mean age of 32 SD 13 years of age (Table 1).
-
A.
Analysis of the ileo-colonoscopy data.
-
All patients underwent MR enterography and ileo-colonoscopy for assessment of inflammatory bowel diseases.
-
Out of the 30 cases, 12 cases were finally diagnosed as Crohn's disease (CD) and 18 cases were diagnosed as ulcerative colitis (UC) in Table 2.
-
Among the included patients, ileo-colonoscopy findings were as follows: Length of the affected part of the intestine was 48.2 ± 44.5 cm SD, mural thickening could not be assessed (NA), mucosal edema was reported in 18 cases (60%), and loss of vascular pattern was reported in 6 cases) (20%).
-
The affected parts of the intestine as detected by ileo-colonoscopy were mainly at descending colon and recto-sigmoid in (6/30, 20%) of cases each, the whole colon in (4/30, 13.3%) of cases, terminal ileum and ileocecal junction in (4/30, 13.3%) of cases, followed by distal ileum that was affected in (3/30, 9.9%) of cases, as well as the anal canal, ascending colon, sigmoid and transverse colon where each of them was affected in (1/30, 3.3%) of cases. The remaining (3/30, 9.9%) cases had no specific lesions (Fig. 1).
-
Diverticular outpouching was only reported in 1 case (3.3%), pseudo-polyps/polyps in 5 cases (16.7%), and backwash ileitis in 5 cases (16.7%); however, erosions/ulcers were reported in 18 cases (60%), skip lesions in 1 case (3.3%), stricture/narrowing in 4 cases (13.3%), mass lesion in 1 case (3.3%), fistulous/sinus tract in 2 cases (6.7%), fat smudging in 0 cases (NA), stagnation (fecal sign/fluid level/gaseous distension) in 0 cases (NA), intestinal obstruction in 0 cases (NA), perforation or leakage in 0 cases (NA), air under the diaphragm in 0 cases (NA), abscess formation in 0 cases (NA), related vascular congestion in 0 cases (NA), related lymphadenopathy in 0 cases (NA), and ascites in 0 cases (NA).
Table 2 Distributions of diseases under follow-up Fig. 1 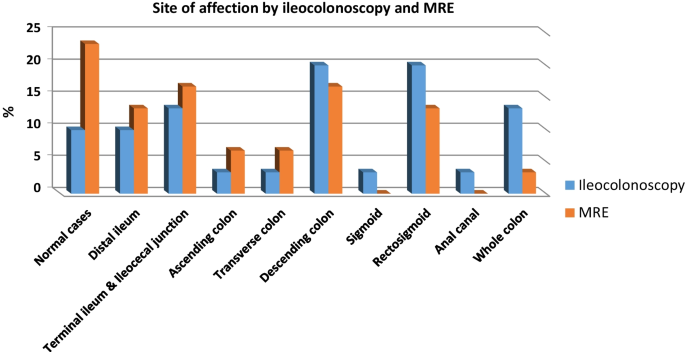
Site of affection by ileo-colonoscopy and MRE
-
-
B.
MRE findings.
-
1.
The length of the affected part of the intestine was 15.8 ± SD 19.7 cm, and mural thickening that was only assessed by MRE showed a mean of 4.1 ± SD 5.1 mm.
-
2.
The affected parts of intestine as detected by MRE were mainly at the ileocecal region (5/30, 16.7%) of cases and descending colon (5/30, 16.7%) of cases, followed by distal ileum (4/30, 13.3%) of cases, recto-sigmoid (4/30, 13.3%) of cases, (2/30, 6.7%) were present in the ascending colon, and transverse colon each and (1/30, 3.3%) was affecting the whole colon. The remaining (7/30, 23.3%) had no specific lesions detected by MRE (Fig. 1).
-
3.
Diverticular outpouchings were only reported in 1 case (3.3%), pseudo-polyps/polyps in 1 case (3.3%), backwash ileitis in 5 cases (16.7%), fat smudging in 4 cases (13.3%), skip lesions in 1 case (3.3%), stagnation (fecal sign/fluid level/gaseous distension) in 3 cases (10%), stricture/narrowing in 3 cases (10%), mass lesion in 2 cases (6.7%), fistulous/sinus tract in 2 cases (6.7%), abscess formation in 1 case (3.3%), related vascular congestion in 2 cases (6.7%), related lymphadenopathy in 22 cases (73.3%); however, erosions/ulcerations were reported in 0 cases (NA), intestinal obstruction in 0 cases (NA), air under the diaphragm in 0 cases (NA), perforation or leakage in 0 cases (NA), and ascites in 0 cases (NA).
-
1.
-
C.
MRE findings were compared to those of ileo-colonoscopy and were documented according to their frequency and percentages in Table 3 (Figs. 2 and 3). P values were calculated for each finding.
-
1.
Ileo-colonoscopy was significantly higher as compared to MRE in the detection of erosions and ulcerations that were only detected by ileo-colonoscopy in (18/30, 60%) of cases versus (0/30, 0%) of cases by MRE, with p value 0.0001.
-
2.
MRE was significantly higher than ileo-colonoscopy in the detection of abscess formation and lymphadenopathy which were only detected by MRE in (1/30, 3.3%) and (22/30, 73.3%), respectively, versus (0/30, 0%) by ileo-colonoscopy, with p value 0.0001 in Figures 4 and 5, respectively.
-
3.
There was a concordance of findings between MRE and ileo-colonoscopy with p values > 0.05 in terms of: mucosal enhancement/hyperemia (Figs. 6, 7 and 8) as they were detected by MRE in (15/30, 50%) versus (18/30, 60%) by ileo-colonoscopy, loss of vascular/haustral pattern (Fig. 7) as they were detected by MRE in (5/30, 16.7%) versus (6/30, 20%) by ileo-colonoscopy, pseudo-polyps/polyps (Fig. 9) were detected by MRE in (1/30, 3.3%) versus (5/30, 16.7%) by ileo-colonoscopy, backwash ileitis (Fig. 8) was equally detected by MRE and ileo-colonoscopy (5/30, 16.7%), fat smudging (Fig. 10) was only detected by MRE (4/30, 13.3%) versus (0/30, 0%) by ileo-colonoscopy, skip lesions (Fig. 10) were equally detected by MRE and ileo-colonoscopy (1/30 3.3%), stagnation represented by fecal sign, fluid level, and gaseous distension (Fig. 4) were only detected by MRE in (3/30, 10%) versus (0/30, 0%) by ileo-colonoscopy, stricture/narrowing (Fig. 8) was detected by MRE in (3/30, 10%) versus (4/30, 13.3%) by ileo-colonoscopy, mass lesions (Fig. 4) were identified by MRE in (2/30, 6.7%) versus (1/30, 3.3%) by ileo-colonoscopy, fistulous/sinus tracts (Figs. 6 and 10) were equally detected by MRE and ileo-colonoscopy (2/30, 6.7%), and related vascular congestion (comb sign) (Fig. 6) was only detected by MRE (2/30, 6.7%) versus (0/30, 0%) by ileo-colonoscopy.
-
4.
There were not any cases of intestinal obstruction, perforation/leakage, air under the diaphragm, and ascites.
Table 3 Comparison between MRE and ileo-colonoscopy findings Fig. 2 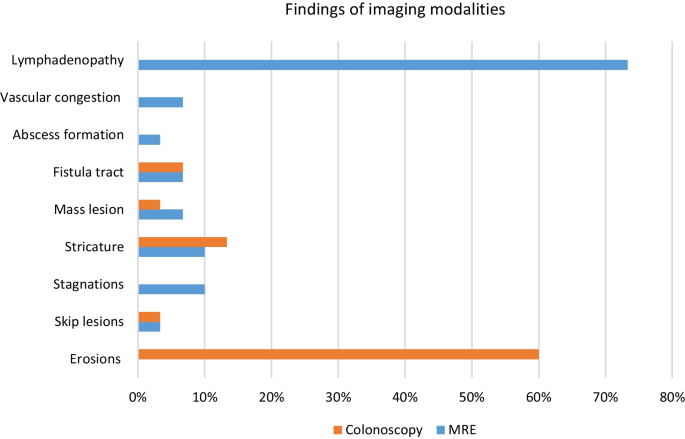
Comparison of features detected by imaging modalities (part 1)
Fig. 3 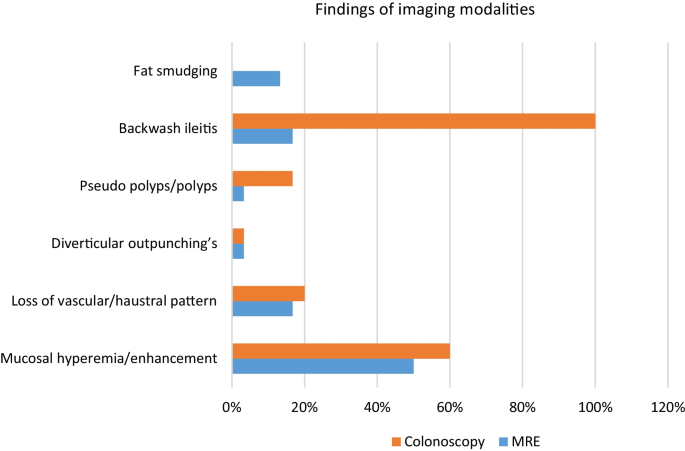
Comparison of features detected by imaging modalities (part 2)
Fig. 4 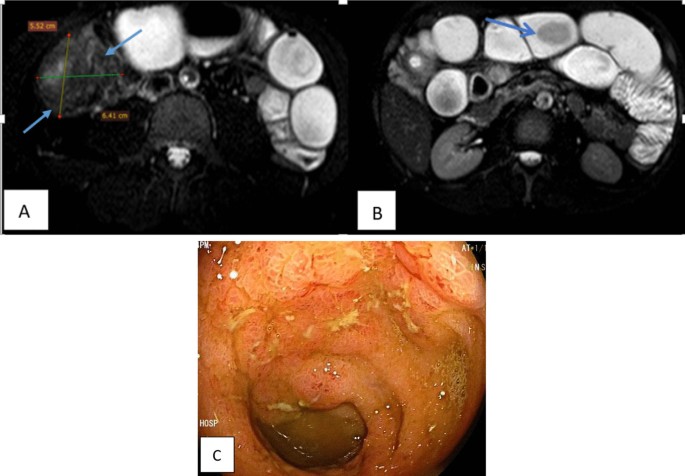
A 38-year-old male patient, known with Crohn’s disease for 8 years on immunosuppressant (methotrexate), presented with abdominal pain for follow-up. A, B Axial T2-w SPAIR images show circumferential mural thickening at the ileocecal junction forming a mass lesion that measures 5.5 × 6.4 cm (as seen in A) with subsequent small-bowel dilatation and stagnation (fecal sign), which is seen at the arrow in B. Ileo-colonoscopy C showed: edematous mucosa of the caecum and ascending colon, as well as edematous mucosa of the ileum with superficial ulcers and multiple small sessile polyps
Fig. 5 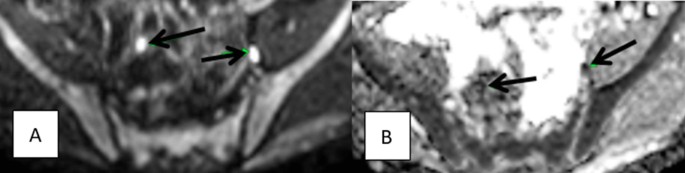
A 20-year-old male patient, known with Crohn's disease for 6 years on Infliximab (Remicade), presented with recurrent diarrhea and abdominal pain for follow-up. A, B Axial DWI b 800 and its ADC map, respectively, show prominent ileocolic and ileac lymph nodes with a hyperintense signal on DWI b images and restricted diffusion on ADC maps (arrow). Ileo-colonoscopy showed swollen ileocecal valve
Fig. 6 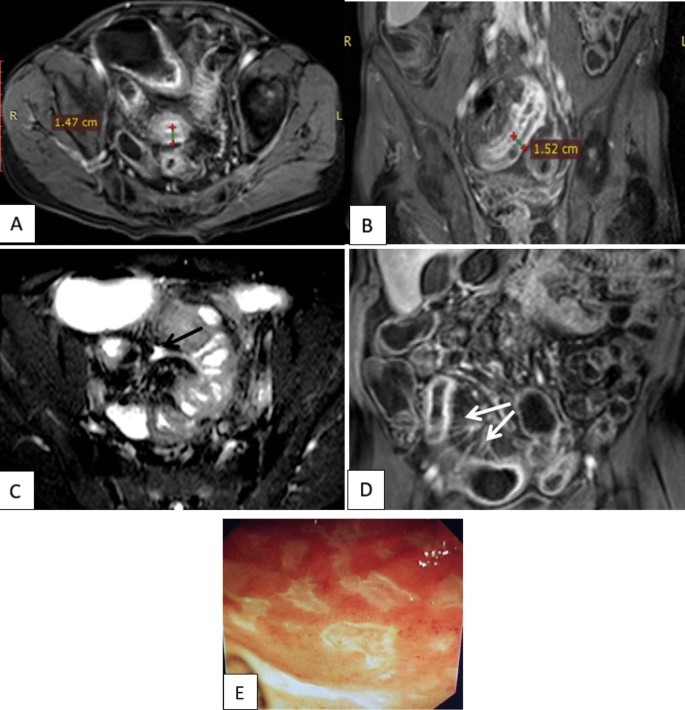
A 45-year-old male patient, known with Crohn's disease for 2 years on mesalazine (Pentasa) and steroids, presented with persistent diarrhea for follow-up. Axial and coronal post-contrast THRIVE images A, B show circumferential mural thickening and trilaminar pattern of enhancement at the distal ileal loop, axial T2-w SPAIR image C shows a short fistulous tract connected to the aforementioned loop (arrow) and coronal post-contrast THRIVE image D shows vascular congestion at the mesenteric side of an ileal loop (Comb sign). Ileo-colonoscopy E showed hyperemic ileal mucosa with patchy linear scarring
Fig. 7 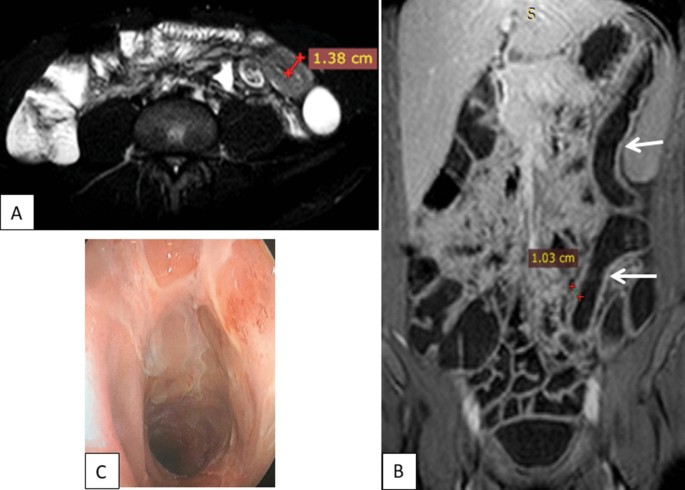
A 36-year-old male patient, known to have ulcerative colitis disease for 7 years on steroids, presented with diarrhea for follow-up. Axial T2-w SPAIR image A shows a segment of mild uniform mural thickening at descending colon, coronal post-contrast THRIVE B loss of normal haustral pattern seen at the descending and sigmoid colon with associated mural thickening and hyperenhancement (arrows). Ileo-colonoscopy C showed marked hyperemia of the mucosa of the recto-sigmoid region with loss of normal vascular pattern of recto-sigmoid region mucosa and multiple superficial ulcerations
Fig. 8 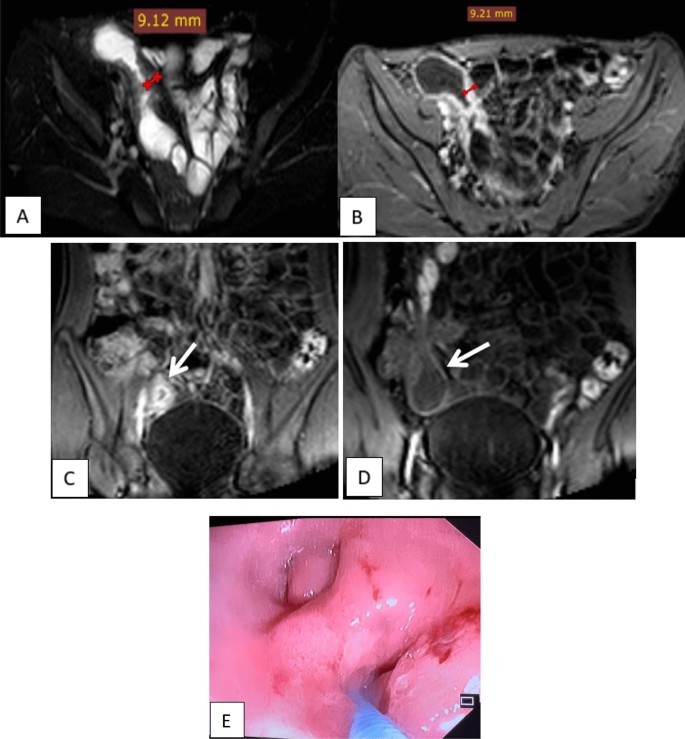
A 22-year-old male patient, known to have Crohn's disease for 4 years on immunosuppressant (methotrexate), presented to the IBD clinic for follow-up. Axial T2-w SPAIR image A shows segmental mural thickening seen at the distal ileum and ileocecal junction, axial post-contrast THRIVE image B shows corresponding mural thickening and hyperenhancement seen at distal ileum and ileocecal junction and C, D coronal post-contrast THRIVE image showing corresponding mural thickening and hyperenhancement seen at distal ileum and associated backwash ileitis at the terminal ileum (arrow). Ileo-colonoscopy E showed multiple superficial ulcers at the caecum and ileocecal valve which is seen edematous and scope cannot pass through it
Fig. 9 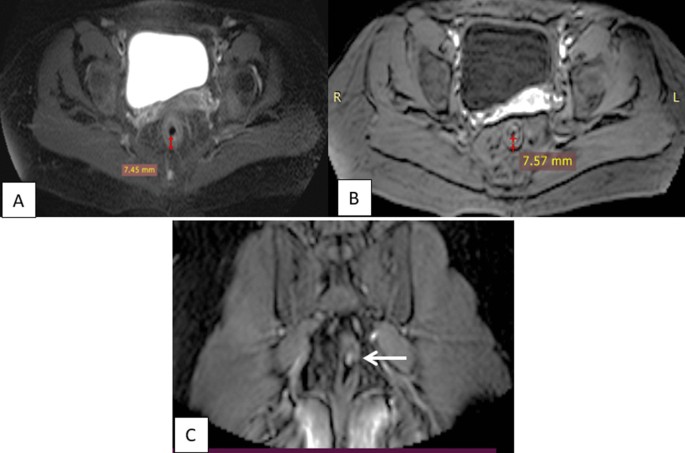
A 41-year-old female patient, known ulcerative colitis disease for 5 years on mesalazine (Pentasa) and steroids, presented with bleeding per rectum and tenesmus for follow-up. Axial T2-w SPAIR A shows mild circumferential uniform rectal mural thickening, axial post-contrast THRIVE image B shows corresponding rectal mural thickening and hyperenhancement, and coronal post-contrast THRIVE image C shows corresponding rectal mural thickening and hyperenhancement with a small polyp seen (arrow). Ileo-colonoscopy showed mild ulcerative proctosigmoiditis with 2 small polyps and granular mucosa of the rectum
Fig. 10 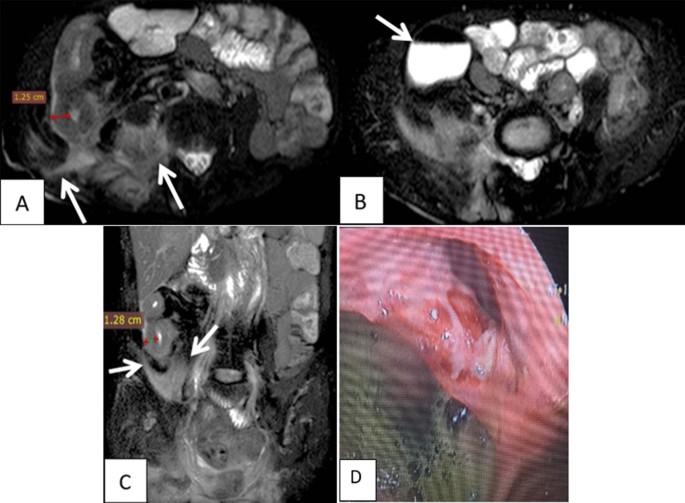
A 52-year-old male patient, known to have Crohn's disease for 15 years on Remicade and Imuran, presented with discharging fistula at the site of ileal resection–anastomosis for follow-up. Axial and coronal T2-w SPAIR images A, C show circumferential mural thickening affecting the distal ileum, with complicating branching fistulous tract, fat smudging and right paraspinal and right psoas inflammation, and impending abscess formation (arrows) and axial T2-w SPAIR (B) image showing fluid level within a skipped area which is noted at caecum (arrow). Ileo-colonoscopy D showed ulcers around the site of ileal anastomosis and cobblestoning features of terminal ileal mucosa
-
1.
-
D.
Paired comparison between the results of MRE and ileo-colonoscopy was done using Wilcoxon sign rank test after normality testing and the McNamara test. The paired comparison shown in Table 4 showed that ileo-colonoscopy had a higher detection rate of diseased areas in (27/30, 90%) of cases as compared to (23/30, 76.7%) of cases by MRE, while MRE has detected a higher number of normal cases (7/30, 23.3%) as compared to ileo-colonoscopy which has detected only (3/30, 10%) cases with no findings. However, this difference was not significant between both modalities with a P value of 0.12.
Table 4 Comparison between results of MRE and ileo-colonoscopy -
E.
Diagnostic indices of MRE in the detection of diseased areas and their confidence interval are shown in Table 5, and MRE has detected the diseased areas with 88.5% sensitivity, 75% specificity, 95.8% positive predictive value, 50% negative predictive value, and 86.7% overall diagnostic accuracy.
Table 5 Diagnostic indices of MRE versus colonoscopy










Comparison of MRE versus ileo-colonoscopy in the detection of disease exacerbation
-
I.
Mucosal hyperemia/edema by ileo-colonoscopy versus mucosal/mural enhancement by MRE (Table 6).
Paired comparison of mucosal enhancement by MRE and mucosal hyperemia by ileo-colonoscopy showed that there is a moderate concordance between results of MRE and ileo-colonoscopy regarding mucosal hyperemia/enhancement between both modalities with p value 0.50 (Table 6); however, the diagnostic indices of MRE versus colonoscopy in terms of mucosal affection showed that MRE had a sensitivity 80% and specificity 60% in detecting mucosal affection (Table 7).
-
II.
Mural thickening
Ileo-colonoscopy was not able to estimate mural thickening at all, while MRE could estimate the mural thickening with a mean of 4.1 ± 5.1 mm SD.
-
III.
Mucosal erosions and ulcerations
Mucosal erosions and ulcerations could not be detected by MRE at all, while ileo-colonoscopy could detect 18/30 cases (60%) with mucosal erosions and ulcerations.
-
IV.
Related lymphadenopathy
Ileo-colonoscopy was not able to detect any related lymphadenopathy when compared to MRE which detected 22/30 cases.
Discussion
Inflammatory bowel disease (IBD) includes both Crohn's disease (CD) and ulcerative colitis (UC). In comparison with the general population, it primarily affects young people, significantly affecting their quality of life and raising morbidity [15].
MRE is useful to assess bowel inflammation and complications such as perforation, fibrosis, and stenosis during the disease course [16].
The current study had a mean patient age of 32 years, which agrees with most of the evidence published in the literature that IBD had a peak incidence during the second and third decades of life with a rare incidence in the 6th decade of life [17].
The affected parts of the intestine as detected by MRE were mainly ileocecal junction in (5/30, 16.7%) cases and descending colon in (5/30, 16.7%), followed by distal ileum in (4/30, 13.3%) and recto-sigmoid in (4/30, 13.3%) cases.
These findings are agreeing with Esmat et al. [18], who found that the most commonly affected part of the colon in patients diagnosed with UC is mainly the left-sided colon (65%) followed by the recto-sigmoid area (18.5%) and finally whole colon (16.3%) as reported by Egyptian gastroenterologists. Also, Petagna et al. [19] have stated that CD mainly affects the ileocecal junction followed by the distal ilium, and this agrees with many authors who correlated the extent of affection of ileum with CD as a part of its pathogenesis where it affects the Peyer's patches which defined as a group of lymphoid follicles in the mucous membrane that lines the small intestine.
In the present study, MRE showed advancement in the assessment of the length of the affected loop of the intestine which was significantly higher in colonoscopy with a mean of 48 ± SD 44 cm versus 15.8 ± SD 19.7 cm, with a p value of 0.0001. We assume that the higher length of ileo-colonoscopy is not as accurate as MRE.
There was a concordance of findings between both imaging modalities in terms of: mural enhancement/hyperemia, loss of haustral/vascular pattern, polyps/pseudo-polyps, backwash ileitis, fat smudging, skip lesions, stagnation, stricture/narrowing, mass lesions, fistulous tracts, perforation, and related vascular congestion with p values > 0.05 each.
Mucosal edema/hyperemia was reported in (18/30, 60%) of cases by ileo-colonoscopy, and this was corresponding to mucosal edema/hyperenhancement in MRE which was reported in (15/30, 50%) of cases; however, this difference was not statistically significant with P value 0.50.
Loss of vascular and haustral pattern was reported in (6/30, 20%) of cases by ileo-colonoscopy, while it was only detected in (5/30, 16.7%) of cases by MRE with one false-negative case; however, this difference was not statistically significant with P value 1.0.
In the present study, MRE was defective in the detection of mucosal lesions, such as pseudo-polyps and polyps as MRE only reported (1/30, 3.3%) cases with pseudo-polyps, while ileo-colonoscopy was positive in (5/30, 16.7%) cases; however, this difference was not statistically significant with p value 0.12.
In the present study, extraluminal affection such as fat smudging, abscess formation, related vascular congestion, and regional lymphadenopathy was only detected by MRE in (4/30, 13.3%), (1/30, 3.3%), (2/30, 6.7%), and (22/30, 73.3%) of cases, respectively, versus no cases by colonoscopy with p value 0.0001 for the abscess formation and the regional lymphadenopathy, and P value 0.12 and 0.50 for fat smudging and related vascular congestion, respectively. Agreeing with Kim et al. [20] as they have mentioned that MRE is a noninvasive diagnostic tool that assesses both small and large bowel affection in IBD, as well as, can identify intraluminal and extraluminal adverse events. And with Langan et al. [21], who have stated that although endoscopy has distinct advantages, it cannot be used to assess extraintestinal abnormalities and can be limited when strictures impede the passage of the endoscope and thus prevent completion of the examination.
According to Neumann et al. [22] who had added that in addition to the lack of extraintestinal visualization using ileo-colonoscopy, as it is mainly limited to the luminal visualization, standard endoscopy may have technical restrictions that hinder the examination of all colon hidden parts. This is because traditional endoscopes only have a 170° field of view due to the use of a complementary metal oxide semiconductor (CMOS) or charge-coupled device (CCD) optics. New developments have been made to improve visualization using seven light-emitting diodes. Particularly, the FUSE colonoscopy's multiple CCD chips, which enable a field of view of up to 330°.
In the present study, paired comparison of both modalities showed that ileo-colonoscopy had a higher detection rate of diseased areas than detected by MRE; however, this difference was not significant with a p value of 0.12. MRE showed a sensitivity of 88.5%, a specificity of 75%, a negative predictive value of 95.8%, a positive predictive value of 50%, and overall diagnostic accuracy of 86.7% in detecting diseased areas within the intestine.
These results are confirmed by a large prospective study conducted by Taylor et al. [23] in the UK where they included all patients diagnosed with IBD and they were assessed using conventional ileo-colonoscopy, MRE, and ultrasound. Results showed that the sensitivity of MRE in the detection of IBD is 97% and for detection of the extent of the disease is 80%; however, specificity in the detection of disease extent was 95% which was higher than reported in our study.
Monitoring the patient's reaction to anti-inflammatory treatment is another possible application for MRE, which would allow for more accurate and less invasive ways of surveillance [24].
Due to the failure of prior therapeutic methods to alter the course of CD, novel therapeutic objectives such as early intervention with effective treatment, treat to target, tight disease control, and surveillance can help patients achieve improved outcomes. These objectives involve regular and timely patient evaluations to monitor clinical (Patient Reported Outcomes, PRO), endoscopic (mucosal healing), and radiographic outcomes so that proactive therapy can be optimized [4].
There was a progression in radiologic evaluation from barium enema investigations to advanced cross-sectional imaging procedures like MR enterography. Endoscopy and magnetic resonance (MR) enterography are complementing diagnostic procedures for the evaluation of inflammatory bowel disease (IBD), as stated by Sahi et al. [25], and Gallego et al. [26]. It has been demonstrated that MR enterography correlates well with endoscopy in predicting disease activity, particularly in Crohn's disease.
Importantly, a higher risk of complications may exist even with lower cumulative radiation exposures [27]. Therefore, imaging techniques that are not using ionizing radiation, such as MRE, are especially appealing in a population of young patients who are susceptible to recurrent imaging [28].
According to Lanier et al. [16], magnetic resonance enterography (MRE) has become the imaging modality of choice for the assessment of IBD activity in both adults and children.
A systematic review and meta-analysis on the role of MRI in the detection of Crohn's disease activity concluded its effectiveness as an alternative to CT enterography as it has good diagnostic accuracy without radiation exposure [29].
The most important findings that detect disease exacerbation and activity are: mucosal hyperenhancement/hyperemia, mural thickening, related lymph node enlargement, and mucosal erosions/ulcerations as well as related vascular congestion of the mesenteric arteries [30,31,32,33].
Mucosal hyperemia/enhancement was detected by MRE with a sensitivity of 80% and specificity of 60%. MRE could estimate the mural thickening with a mean of 4.1 ± SD 5.1 mm. Yet, mural thickening could not be detected by ileo-colonoscopy at all, with a significant difference; the p value was 0.001.
In the current study, MRE could detect related lymphadenopathy in (22/30, 73.3%) cases versus (0/30, 0%) cases by ileo-colonoscopy with a significant difference of P value of 0.0001. DWI was useful in the detection of lymphadenopathy, which is an important marker of disease exacerbation; lymph nodes with restricted DWI were of good value in the detection of the active inflammatory process. According to the literature, DWI with parallel imaging permits the detection of inflammation in Crohn's disease patients, and the lower ADC values in the inflamed bowel segments indicate restricted diffusion [34].
However, mucosal erosions and ulcerations could not be detected by MRE in this study, while using ileo-colonoscopy could detect (18/30, 60%) of cases, with mucosal erosions and ulcerations, versus (0/30, 0%) of cases by MRE, with a significant difference P value 0.0001. According to Sinha et al. [35], superficial aphthous ulcers might appear on T2WI when there is good distention of the lumen. It appears as an intermediate signal on T2WI, surrounded by a focal area of bright T2WI signal. This might have been apparent in UC cases with a lack of proper colonic distension in the MRE. They have also stated that deep ulcers would appear as thin lines penetrating the bowel wall that appears bright in T2 W sequences with fat suppression. These deep ulcers might complicate to become penetrating fistulae [36]. The current study included (2/30, 6.7%) cases with fistulae/sinus tracts that were detected equally by MRE and ileo-colonoscopy.
On the other hand, Dulai et al. [37] have stated that MRE has a low negative predictive value for the detection of mucosal pathology because it may exclude the presence of active inflammation or ulceration when it is present, and further endoscopic assessment may still be necessary for patients with persistent symptoms despite the appearance of normal mucosa on MRE.
Related vascular congestion of the mesenteric arteries (vasa recta) was detected by MRE in (2/30, 6.7%) of cases, while it was not detected by ileo-colonoscopy. With a P value of 0.50, this was described by Tolan et al. [33] as a sign of active illness when combined with intestinal wall edema and enhancement.
Limitations
In the present study, we were limited by the lack of long-term follow-up of patients to assess the patterns of disease activities. Also, we only assessed patients with CD and UC and disregarded patients with idiopathic inflammatory bowel disease, so our results cannot be generalized over all types of IBD.
Our study showed some MRE examination difficulties that include prolonged examination time and patients with associated spine and sacroiliac joint inflammation who have found difficulty in the prolonged supine position during examination.
Although the MRE was reported by an expert radiologist with 12 years of experience in GIT sub-specialty who was blinded to the ileo-colonoscopy results, it would have been better if it was reported by two radiologists.
Recommendations
The use of 3 T MR operators will provide a more reasonable evaluation for dynamic contrast-enhanced and diffusion-weighted MR images to better detect active versus chronic stages of the disease. It will also allow a faster scanning time about 15–20 min rather than the standard 30–60 min while utilizing a 1.5 T MR operator.
Conclusions
MRE is sensitive, inexpensive, noninvasive, and radiation-free for inflammatory bowel disease detection, with 86.7% diagnostic accuracy for affected areas. Unlike ileo-colonoscopy, it could examine the entire small intestine, precisely measure the affected loop, and detect activity signs such as mural thickening and lymphadenopathy. However, ileo-colonoscopy is useful in assessing the large intestine and terminal ileum in IBD patients, and it was superior in detecting mucosal erosions and superficial ulcers. IBD treatment protocols should incorporate MRE for small-bowel, colonic, and extra-enteric assessment, monitoring of disease activity, and anti-inflammatory therapy response.
Availability of data and materials
All the data and materials used in the manuscript are available with the corresponding author upon reasonable request.
Abbreviations
- IBD:
-
Inflammatory bowel disease
- GI:
-
Gastrointestinal
- CD:
-
Crohn's disease
- UC:
-
Ulcerative colitis
- STRIDE:
-
Selecting Therapeutic Targets in Inflammatory Bowel Disease
- MRE:
-
Magnetic resonance enterography
- MRI:
-
Magnetic resonance imaging
- IRB:
-
Institutional review board
- ICRID:
-
Integrated Clinical and Research Center for Intestinal Disorders
- NBI:
-
Narrow-band imaging
References
Sandborn WJ, Hanauer S, Van Assche G (2014) Treating beyond symptoms with a view to improving patient outcomes in inflammatory bowel diseases. J Crohns Colitis 8:927–935
Ng SC, Shi HY, Hamidi N (2018) Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet 390(10114):2769–2778
Fiorino G, Peyrin-Biroulet L, Danese S (2012) Bowel damage assessment in Crohn’s disease by magnetic resonance imaging. Curr Drug Targets 13:1300–1307
Peyrin-Biroulet L, Sandborn W, Sands BE (2015) Selecting therapeutic targets in inflammatory bowel disease (STRIDE): determining therapeutic goals for treat-to-target. Am J Gastroenterol 110(9):1324–1338
Panés J, García-Olmo D, Van Assche G (2018) Long-term efficacy and safety of stem cell therapy (Cx601) for complex perianal fistulas in patients with Crohn’s disease. Gastroenterology 154(5):1334-1342.e4
Neurath MF, Travis SPL (2012) Mucosal healing in inflammatory bowel diseases: a systematic review. Gut 61:1619–1635
Froslie KF, Jahnsen J, Moum BA (2007) Mucosal healing in inflammatory bowel disease: results from a Norwegian population-based cohort. Gastroenterology 133:412–422
Bruining DH, Loftus EV Jr, Ehman EC (2011) Computed tomography enterography detects intestinal wall changes and effects of treatment in patients with Crohn’s disease. Clin Gastroenterol Hepatol 9:679–683
Kaushal P, Somwaru AS, Charabaty A (2017) MR enterography of inflammatory bowel disease with endoscopic correlation. Radiographics 37(1):116–131
Kim YG, Jang BI (2013) The role of colonoscopy in inflammatory bowel disease. Clin Endosc 46(4):317–320
Varyani F, Samuel S (2019) Can MRE replace ileo-colonoscopy for evaluating disease activity in Crohn’s disease. Best Pract Res Clin Gastroenterol 38:101621
Somwaru AS, Khanijow V, Katabathina VS (2019) Magnetic resonance enterography, colonoscopy, and fecal calprotectin correlate in colonic Crohn’s disease. BMC Gastroenterol 19:1–19
Somwaru AS, Khanijow V, Katabathina VS (2019) Magnetic resonance enterography, colonoscopy, and fecal calprotectin correlate in colonic Crohn’s disease. BMC Gastroenterol 19:210
Yoon K, Chang K-T, Lee HJ (2015) MRI for Crohn’s disease: present and future. Biomed Res Int 2015:1–9
De Mattos BR, Garcia MP, Nogueira JB (2015) Inflammatory bowel disease: an overview of immune mechanisms and biological treatments. Mediat Inflamm 493012(1155):2015
Lanier MH, Shetty AS, Salter A (2018) Evaluation of noncontrast MR enterography for pediatric inflammatory bowel disease assessment. J Magn Reson Imaging 48(2):341–348
Abraham C, Cho JH (2009) Inflammatory bowel disease. N Engl J Med 361(21):2066–2078
Esmat S, El Nady M, Elfekki M (2014) Epidemiological and clinical characteristics of inflammatory bowel diseases in Cairo, Egypt. World J Gastroenterol WJG 20(3):814
Petagna L, Antonelli A, Ganini C (2020) Pathophysiology of Crohn’s disease inflammation and recurrence. Biol Direct 15(1):1–10
Kim KJ, Lee Y, Park SH (2015) Diffusion-weighted MR enterography for evaluating Crohn’s disease: how does it add diagnostically to conventional MR enterography. Inflamm Bowel Dis 21(1):101–109
Langan RC, Gotsch PB, Krafczyk MA (2007) Ulcerative colitis: diagnosis and treatment. Am Fam Physician 76(9):1323–1330
Neumann H, Tontini GE, Albrecht H (2016) Su1702 accuracy of the full spectrum endoscopy system (FUSE) for prediction of colorectal polyp histology. Gastrointest Endosc 83(5):AB402
Taylor SA, Mallett S, Bhatnagar G (2018) Diagnostic accuracy of magnetic resonance enterography and small bowel ultrasound for the extent and activity of newly diagnosed and relapsed Crohn’s disease (METRIC): a multicentre trial. Lancet Gastroenterol Hepatol 3(8):548–558
Sempere GA, Martinez Sanjuan V (2005) MRI evaluation of inflammatory activity in Crohn’s disease. AJR Am J Roentgenol 184:1829–1835
Sahi KS, Lee KS, Moss A (2015) MR enterography of the ileoanal pouch: descriptive radiologic analysis with endoscopic and pathologic correlation. AJR Am J Roentgenol 205(5):W478–W484
Gallego JC, Echarri AI, Porta A (2011) Ileal Crohn’s disease: MRI with endoscopic correlation. Eur J Radiol 80(2):e8–e12
Brenner DJ, Doll R, Goodhead DT (2003) Cancer risks attributable to low doses of ionizing radiation: assessing what we really know. Proc Natl Acad Sci USA 100:13761–13766
Amitai MM, Ben-Horin S (2013) Magnetic resonance enterography in Crohn’s disease: a guide to common imaging manifestations for the IBD physician. J Crohn’s Colitis 7(8):603–615
Ahmad R, Ajlan AM, Eskander AA (2021) Magnetic resonance imaging in the management of Crohn’s disease: a systematic review and meta-analysis. Insights Imaging 12:118
Knuesel PR, Kubik RA, Crook DW (2010) Assessment of dynamic contrast enhancement of the small bowel in active Crohn’s disease using 3D MR enterography. Eur J Radiol 73:607–613
Gourtsoyiannis N, Grammatikakis J, Papamastorakis G (2006) Imaging of small intestinal Crohn’s disease: comparison between MR enteroclysis and conventional enteroclysis. Eur Radiol 16:1915–1925
Sinha R, Rajiah P, Ramachandran I (2013) Diffusion-weighted MR imaging of the gastrointestinal tract: technique, indications, and imaging findings. Radiographics 33:655–676
Tolan DJ, Greenhalgh R, Zealley IA (2010) MR enterographic manifestations of small bowel Crohn disease. Radiographics 30:367–384
Oto A, Zhu F, Kulkarni K (2009) Evaluation of diffusion-weighted MR imaging for detection of bowel inflammation in patients with Crohn’s disease. Acad Radiol 16(5):597–603
Sinha R, Murphy P, Sanders S (2013) Diagnostic accuracy of high-resolution MR enterography in Crohn’s disease: comparison with surgical and pathological specimen. Clin Radiol 68:917–927
Sinha R, Verma R, Verma S (2011) MR enterography of Crohn disease: Part 2, imaging and pathologic findings. AJR Am J Roentgenol 197:80–85
Dulai PS, Levesque BG, Feagan BG (2015) Assessment of mucosal healing in inflammatory bowel disease. Gastrointest Endosc 82(2):246–255
Acknowledgements
We acknowledge the Integrated Clinical and Research Centre for Intestinal Disorders (ICRID) for referring IBD patients to our radiology department for MRE.
Funding
No funding was received for performing this study.
Author information
Authors and Affiliations
Contributions
MYA and AFAES conceived of the idea for the study. MYA and HS developed the study’s hypothesis. IA obtained full medical histories from the participants and examined participants by colonoscopy. RMMA reported the findings of magnetic resonance enterography (MRE). AFAES collected and analyzed the data. RMMA wrote the manuscript. MYA and HS verified the analytical methods and revised the manuscript critically for important intellectual content. MYA and HS supervised the work. All authors provided critical feedback and helped shape the research, analysis, and final version of the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This prospective study was ethically approved by the “Research and Ethics Committee” (REC) of the faculty of medicine Cairo University hospitals, Number: MS-456-2020. Informed verbal consent was taken from the participants. No additional intervention was needed for the routinely referred MRE protocol applied in Kasr Al-Ainy, Cairo University hospitals.
Consent for publication
No participant's personal information is included in our manuscript, and before publishing, names were taken from all the photographs and figures.
Competing interests
We have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ali, R.M.M., El Salam, A.F.A., Anwar, I. et al. Role of MR enterography versus ileo-colonoscopy in the assessment of inflammatory bowel diseases. Egypt J Radiol Nucl Med 54, 17 (2023). https://doi.org/10.1186/s43055-023-00967-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-00967-5