- Review
- Open access
- Published:
Spectrum of imaging findings in osteoarticular tuberculosis
Egyptian Journal of Radiology and Nuclear Medicine volume 55, Article number: 23 (2024)
Abstract
Background
Tuberculosis (TB) is still a major public health problem. It is endemic in most of the developing countries. Osteoarticular tuberculosis is an uncommon infection, and its diagnosis is often missed due to non-specific clinical and imaging findings.
Main body of abstract
The diagnosis of osteoarticular TB is often delayed due to non-specific clinical presentation and often mimics with other infectious/inflammatory disorders. However, as the disease is curable, prompt diagnosis and early initiation of treatment remain critical to prevent the development of deformity and bone destruction. MRI is sensitive in early detection of articular and marrow abnormalities, detecting complications and assessing response to treatment.
In this review, we describe the spectrum of various MR imaging findings of osteoarticular TB, which helps in early diagnosis and differentiating these from other pathologies with similar imaging appearances. These are described through case-based illustrations of different anatomical locations of osteoarticular TB.
Short conclusion
MR imaging is the emerging modality of choice for early diagnosis of osteoarticular tuberculosis and helps to differentiate it from other infective/inflammatory diseases.
Background
Tuberculosis (TB) can involve pulmonary as well as extra pulmonary sites. Osteoarticular TB accounts for 1–3% cases of all tuberculous infections [1]. Tubercular spondylitis constitutes almost 50% of cases, followed by tubercular arthritis mainly involving peripheral joints in 30% of cases, tubercular osteomyelitis in 19% and remaining 1% which includes tenosynovitis, bursitis and Poncet’s disease. [2, 3]
Osteoarticular tuberculosis is increasing in incidence especially in developing countries due to the AIDS epidemic, emergence of multi-drug-resistant strains of Mycobacterium tuberculosis and growing number of immunocompromised patients [4, 5]. Osteoarticular TB results from hematogenous dissemination of mycobacteria from primary/reactivated focus of infection [6]. Among the various imaging modalities including conventional radiography, ultrasonography, computed tomography and bone scan, MRI is the modality of choice because of its multiplanar capability and excellent soft tissue contrast, which helps in early detection of changes in bones and joints including bone marrow oedema, synovial proliferation, bone and cartilage destruction and soft tissue abnormalities. [7]
In this article, we have described the various patterns of osteoarticular TB and their imaging features on MRI through case-based illustrations. Certain imaging features which point to the diagnosis of TB have been described, and key imaging features which aid in diagnosis and choosing the correct differentials have been highlighted.
Main text
Classification of osteoarticular TB based on anatomical location
Tubercular spondylitis
Spinal TB or Pott’s spine is the most common type of osteoarticular TB. It can occur secondary to pulmonary or abdominal TB and rarely occur as the primary manifestation.
Presentation: Clinical presentation is usually non-specific, but the patients my present with constitutional symptoms, backache, spinal deformity and tenderness among others.
Location: Most common sites of spinal TB are lower thoracic spine followed by lumbar and cervical spine. Involvement of cervical vertebrae (3–5%) and atlantoaxial joint (1%) are less common. Tubercular spondylitis commonly affects two or more contiguous vertebrae; however, skip lesions (4–10%) and single vertebral involvement may occur.
Patterns of vertebral TB: According to anatomical location, vertebral TB is subclassified as paradiscal, anterior, central and posterior arch lesions [8] (Fig. 1).
-
Paradiscal involvement of vertebral end plates adjacent to intervertebral disc and with later disc involvement (Fig. 2).
-
Anterior-anterior subperiosteal lesion under anterior longitudinal ligament, involved multiple contiguous vertebrae (Fig. 3).
-
Central-single vertebral involvement with preservation of adjacent disc spaces (Fig. 4).
-
Posterior/appendiceal-isolated involvement of posterior elements of vertebrae (Fig. 5).

Patterns of vertebral TB [28]

TB spine (paradiscal pattern): A 13-year-old girl with backache and acute onset paraplegia. Radiograph thoracolumbar spine AP view (A) reveals destruction of D5-D6 vertebrae with bilateral paravertebral soft tissue abscesses (white arrowheads). On MRI-sagittal T2 (B) coronal STIR (C) and post-contrast axial (D) images demonstrate wedge collapse of D5–D6 vertebrae with loss of intervening disc space with kyphotic deformity (white circle) and peripherally enhancing collection in pre, paravertebral (arrow) with epidural extension and spinal cord compression (black arrow). After anterolateral decompression, Anti Tubercular Treatment (ATT) was started. HPE image (E) shows caseating epitheloid cell granuloma with langerhans’s giant cells and areas of necrosis along with granulation tissue

TB spine (anterior subligamentous pattern): A 25-year-old female with cough and chest pain. Radiograph thoracolumbar spine AP view (A) reveals bilateral paravertebral soft tissue abscesses (white arrowheads). On MRI- Sagittal T2 (B) and post-contrast sagittal and axial (C, D) images demonstrate large peripherally enhancing pre and paravertebral abscesses (dotted arrow) with epidural extension and spinal cord compression (white arrow). No obvious destruction of any vertebral body and disc space. ATT was started and patient shows significant clinical improvement after 3 month follow-up

TB spine (central pattern)-A 11-year-old girl presented with backache and acute onset paraplegia. Plain radiograph DL spine (A) reveals reduced height of D5 vertebra with adjacent paravertebral soft tissue abscess (blue oval). On MRI-Sagittal T2 (B) show marrow oedema of body D4, D5 and posterior elements of D5 (oval) with concentric collapse of D5 vertebra (dotted arrow) with preservation of adjacent disc spaces. On post-contrast axial image (C) peripherally enhancing pre and paravertebral collection (arrow) with epidural extension (arrowhead), causing narrowing of spinal canal. Patient underwent decompressive surgery and put on ATT and bracing were advised. On follow-up after 4 months patient responded well and able to walk with support

TB spine (posterior element TB)-A 11-year-old girl presented with backache and acute onset paraplegia. Plain radiograph of spine was normal. On MRI- Sagittal STIR (A), axial T2 (B) and post-contrast axial (C) images show marrow oedema involving body of D3 and posterior elements of D2 and D3 vertebrae (oval) with destruction of posterior element with heterogenous enhancement (arrow). Homogenously enhancing posterior epidural collection with narrowing of spinal canal and spinal cord compression (arrowhead). Peripherally enhancing enlarged necrotic conglomerated mediastinal lymph nodal mass (dotted arrow). Findings suggestive of tubercular spondylitis (Posterior type). After decompressive surgery, ATT was started. On follow-up after 3 months patient was able to walk with support
There is no single test available for diagnosis of TB. Combined approach using clinical and demographic history, radiological imaging and microbiological and histopathological investigations are required to reach the final diagnosis. Microbiological culture remains the gold standard test for diagnosis of TB. However, culture results are only available after 6–8 weeks which results in delay in the initiation of treatment.
Radiological imaging
Plane radiography Radiographs are usually the first investigation obtained in patients with suspected TB, but in early stage of disease, radiographs may appear normal. For any radiolucent lesion to be apparent on radiograph, there should be at least 30% loss of bone minerals. [9]
Ultrasonography Ultrasonography although non-specific helps in the assessment of soft tissue abscesses and guidance for drainage.
Computed tomography (CT) scan CT scan is particularly useful for the assessment of degree of bone destruction and presence of sequestrum. Some skeletal location of osteoarticular TB including craniovertebral junction, posterior element of vertebra, ribs, sternum and sacroiliac joints that are not clearly visible on radiographs can be better evaluated by CT scan. [11]
A CT-guided biopsy of lesion in bone/joint is most commonly used method for microbiological and histopathological diagnostic work-up. [12]
MRI characteristics of tubercular spondylodiscitis
-
Bone marrow oedema shows high signal intensity on T2 WI and STIR images.
-
Vertebral lesions appear hypointense on T1WI and hyperintense on T2WI and shows heterogenous post-contrast enhancement (Figs. 2, 3, 4, and 5)
-
Intervertebral disc involvement appears hypointense on T1WI and hyperintense on T2WI and will show heterogeneous post-contrast enhancement (Fig. 6).
-
Pre, paravertebral and psoas abscess appear as heterogenous collections with peripheral enhancement on post-contrast images with central non-enhancing hypointense area. The location and extent of these abscesses can be best demonstrated on post-contrast T1WI images (Figs. 2, 3, and 4).
-
These granulation tissues and epidural abscesses cause narrowing of the thecal sac and compression of the spinal cord resulting in neurological complications [13] (Figs. 3, 4, 5, 6)
-
Tubercular granulomas and meningeal thickening and enhancement the better appreciated on post-contrast T1WI (Fig. 6).
-
Rare sites including craniovertebral junction lesions and skip lesion are also better evaluated with MRI (Fig. 7).

TB meningitis involving brain and spinal cord- A 13-year-old girl presented with backache with history of disseminated TB. On MRI-Sagittal T2, STIR (A, B) and post-contrast sagittal, axial (C, D) images show collapse of D5 vertebra (arrow) and peripherally enhancing anterior subligamentous collection (arrow heads). Spinal canal shows long segment sheath like meningeal thickening and enhancing lesions suggestive of arachnoiditis with exudates (dotted arrows). Few intradural extramedullary enhancing nodules seen likely tuberculomas (black arrow). Axial post-contrast image (E) of brain shows few conglomerated ring enhancing lesions in right basal ganglia and bilateral cingulate gyrus (white oval). Findings suggestive of—Pott’s spine with tubercular meningitis brain and spinal cord. Patient was started on ATT and responded well to treatment

TB craniovertebral junction-A 11-year-old boy presented with swelling over neck region, with neck stiffness. On MRI-Sagittal STIR image (A) show marrow oedema in dens with atlantoaxial subluxation (arrow). Post-contrast axial image (B) shows peripherally enhancing collection anterior to dens (arrow head). Whole spine screening sagittal T2WI (C) shows skip lesion in lumbar region (thick arrow). On post-contrast sagittal and axial images (D, E) show intravertebral (dotted arrow) and prevertebral abscess (black arrow)
Key imaging features suggestive of TB versus other infectious aetiologies include.
-
More than one vertebra involved
-
Relative sparing of intervertebral disc
-
Large paravertebral abscesses
-
Subligamentous spread
-
Heterogenous signal intensity on MRI
-
Rim enhancement pattern of MRI. [14]
Tubercular arthritis
Tubercular arthritis is most common site for extra-axial osteoarticular TB.
Presentation Slowly progressive joint pain and boggy swelling are the most common presentation. In advanced stage of disease, ankylosis may occur. Clinically, tubercular arthritis mimics gout or juvenile arthritis, resulting in delay and confusion in diagnosis. [15]
Location Tuberculous arthritis is usually monoarticular (90%).
Common- Large weight bearing joints, such as knee, hip joint and sacroiliac joint.
Less common-. Shoulder, ankle, elbow and wrist joints (1% each).
Rare- Small joints of hands, feet, acromioclavicular and sternoclavicular joints.
Radiological imaging
Plain radiograph Juxta-articular osteopenia, bone erosions and gradual narrowing of joint space are typical. Phemister triad is characteristic feature of tubercular arthritis, described by Phemister (Figs. 10, 11, 12, 13, 14).
Ultrasonography Ultrasonography can be useful in the detection of joint effusion in cases of tubercular arthritis and soft tissue abscess, psoas abscess associated with other forms of osteoarticular TB; however, it is non-specific.
Computed tomography CT scan is much better in the detection and characterization of lytic and sclerotic bone lesions and destruction of bony circumference compared to plane radiographs. It provides better delineation of shape and calcification of the soft tissue abscesses.
MRI findings in tubercular arthritis:
-
1.
Bone and cartilage changes:
Bone marrow oedema or osteomyelitis associated with tubercular arthritis is the characteristic appearance of marrow oedema on T2/STIR images with variable amount of enhancement on post-contrast images (Figs. 8, 9, 10, 11, 12, 13, 14, 15).
Fig. 8 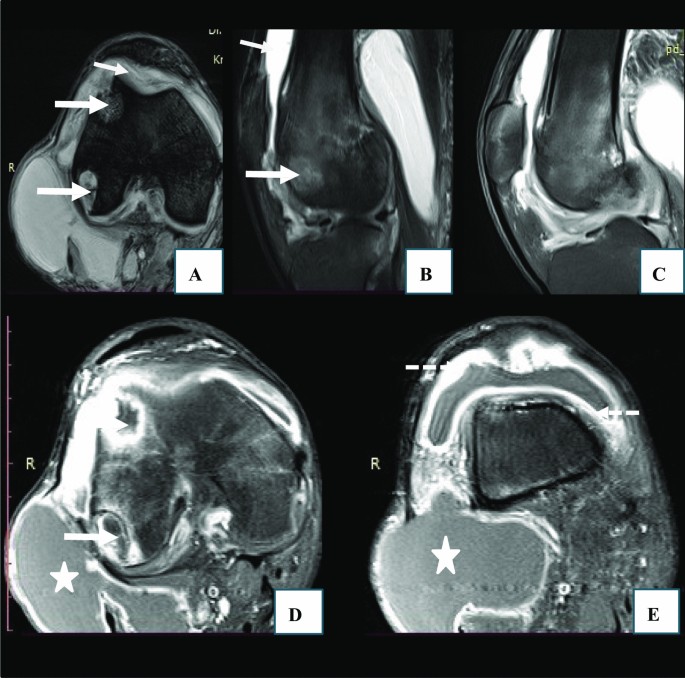
TB knee joint- A 22-year-old male patient presented with complain of pain and swelling around right knee joint since 8 months. On MRI-axial T2 (A), sagittal T2, PD FS (B, C) and post-contrast axial images (D, E) show mild effusion in knee joint and suprapatellar recess (arrows), with thick and enhancing synovial lining (dotted arrows). Few peripherally enhancing juxta-articular marginal erosions seen in distal femur (thick arrows). Another peripherally enhancing collection seen on posterolateral aspect of knee, between joint capsule and biceps femoris tendon, (asterisks). Findings suggestive of infective aetiology likely tubercular. Synovial fluid examination revealed tubercular aetiology
Fig. 9 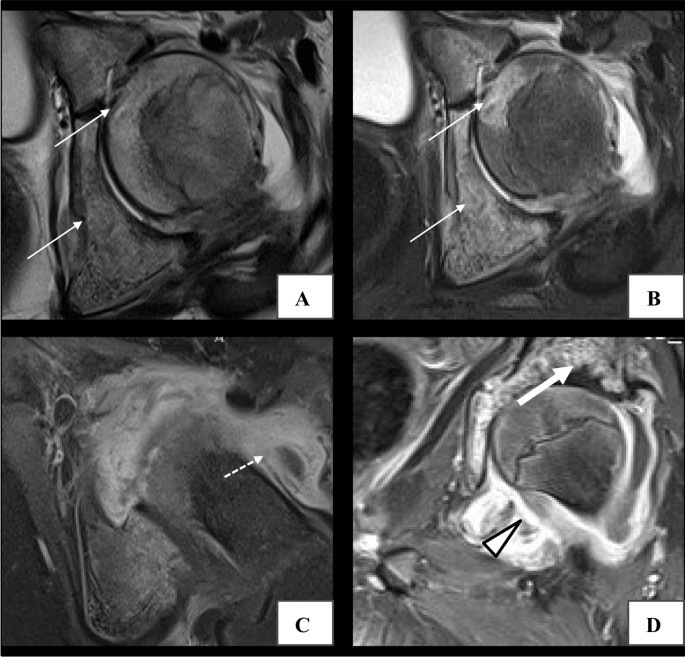
TB hip joint-A 12-year-old boy presented with pain in left hip while walking, with history of CNS tuberculosis. Plain radiograph of left hip joint was normal. On MRI- Axial T2, STIR (A, B), post-contrast axial and coronal (C, D) images show areas of bone marrow oedema in left femoral head and acetabulum (arrows) with small peripherally enhancing periarticular collection (dotted arrow). Marginal erosions in acetabulum (thick arrow) with synovitis (arrowhead). Findings suggestive of infective aetiology likely tubercular. ATT was started and good clinical outcome was noted on follow-up after 6 months
Fig. 10 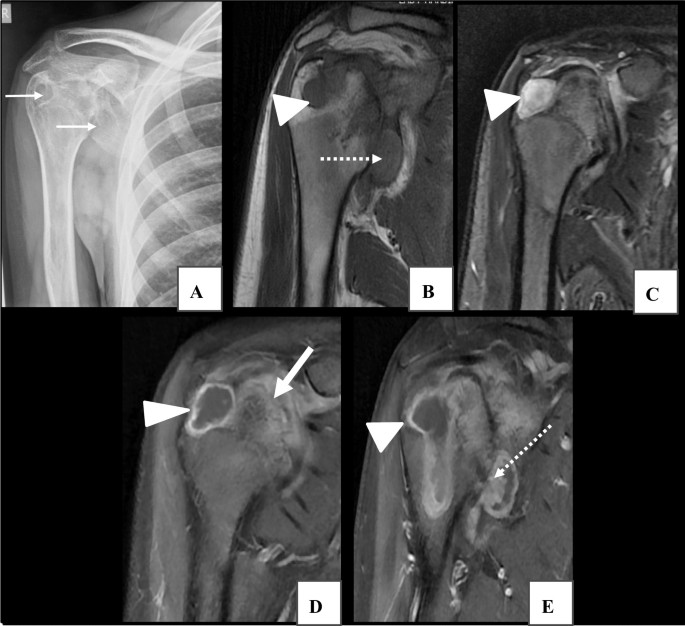
TB shoulder joint- A 30-year-old male presented with chronic pain in right shoulder. Plain radiograph of shoulder (A) reveals few lytic areas and marginal erosions at head of humerus and inferior margin of glenoid (arrows). On MRI-Coronal T1 (B), sagittal T2 (C) and coronal STIR (D) and post-contrast coronal (E, F) images show altered signal intensity areas appearing hypointense on T1, hyperintense on T2/STIR images with smooth peripheral enhancement and central non-enhancing areas suggestive of bone erosions seen involving head of humerus (arrow) and inferior aspect of glenoid (dotted arrow), with cortical irregularity of articular surfaces. Thick and enhancing synovium (thick arrow) with adjacent inflammatory changes. Findings suggestive of infective aetiology likely tubercular. On follow-up after 3 months of ATT, clinical improvement was seen
Fig. 11 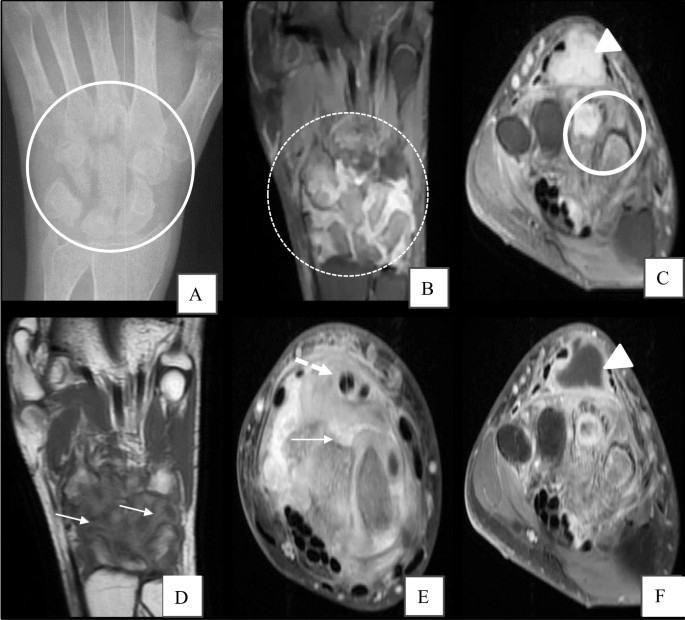
TB wrist joint with tenosynovitis-A 18-year-old male patient presented with pain and swelling over right wrist since 4 months. Plain radiograph wrist (A) reveals marginal erosions involving all carpal bones, base of 4th 5th metacarpal and erosion and destruction of base of 3rd metacarpal bone (oval). On MRI- PD FS coronal (B), axial (C), coronal T1 (D) and post-contrast axial (E, F) images reveal marginal erosions and bone marrow oedema involving all carpal bones (dotted oval) and base of 2nd, 3rd metacarpal (thick oval). Diffuse synovial thickening and enhancement suggestive of synovitis (arrows) also extending along tendon sheath suggestive of tenosynovitis (dotted arrow). Peripherally enhancing synovial collection at dorsum of hand (arrowhead). Findings suggestive of tubercular arthritis of wrist and hand. On follow up after 3 months of ATT, resolution of pain and swelling was noted
Fig. 12 
TB ankle joint- A 35-year-old female patient presented with pain and swelling around ankle joint since 3 months. Plain radiograph of ankle joint (A) shows joint space widening with lytic area in distal epiphysis and metaphysis of fibula (arrow) with adjacent soft tissue swelling. On MRI-Coronal PD FS (B) shows joint effusion at ankle and talocalcaneal joints. Sagittal T2 (C) and post-contrast axial (D, E) images show altered signal intensity area with post-contrast enhancement seen in distal metaphysis of fibula (oval). Thick enhancing synovium extending along tendon sheaths (arrow) with small peripherally enhancing collection (arrowhead) on lateral aspect of foot. Findings suggestive of infective aetiology likely tubercular arthritis. On follow-up, patient responded well to anti-tubercular treatment
Fig. 13 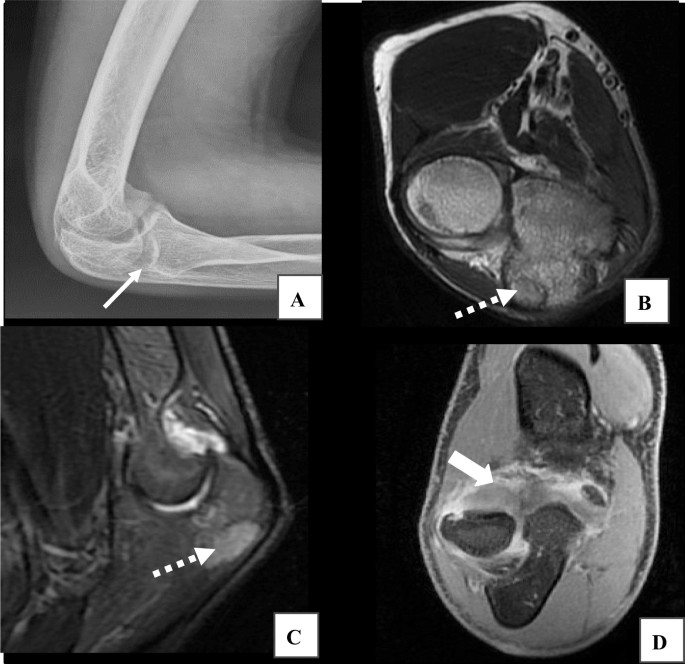
TB elbow joint- A 14-year-old boy presented with pain and swelling around left elbow. Plain radiograph elbow joint (A) shows small lytic area in olecranon process of ulna (arrow). On MRI- Axial T2 and sagittal STIR images (B, C) show areas of bone marrow oedema in olecranon process of ulna (dotted arrow) with mild joint effusion. Post-contrast coronal image (D) shows thick enhancing synovium with periarticular inflammatory changes (thick arrow). Findings suggestive of infective aetiology likely tubercular. ATT was started, clinical improvement was seen on follow-up imaging after 6 months
Fig. 14 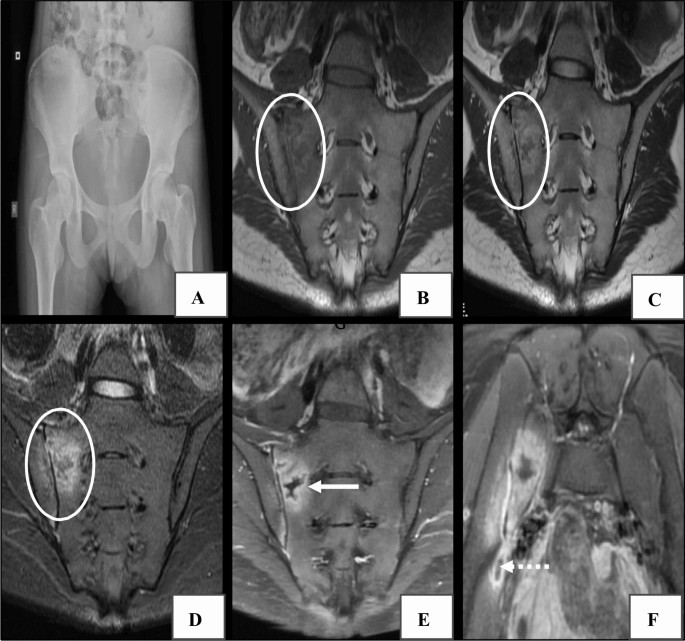
TB sacroiliitis-A 12-year-old girl with history of disseminated Koch's presented with low backache. Radiograph of lumbosacral spine was normal. Plain AP radiograph of pelvis (A) reveals no significant abnormality. On MRI- Coronal T1, T2 and STIR (B, C and D) and post-contrast coronal and axial (E, F) images show altered signal intensity area with surrounding subarticular bone marrow oedema (white oval), showing peripheral enhancement (arrow) seen involving periarticular region of right sacroiliac joint (right sacral ala, lateral mass and ileum). Peripherally enhancing soft tissue abscess (dotted arrow). Findings suggestive of tubercular sacroiliitis. Patient was started on ATT. On follow-up after 5 months of treatment, clinical condition was improved
Fig. 15 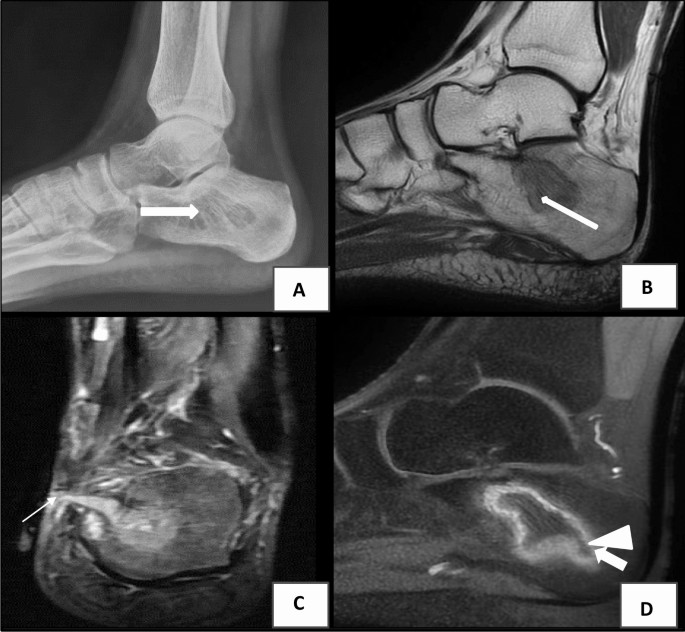
TB osteomyelitis calcaneum-A 18-year-old male presented with chronic discharging sinus over medial aspect of right foot. Plain radiograph of foot (A) shows well-defined lytic lesion without sclerotic rim seen in body of calcaneum, posteriorly (thick arrow). On MRI- sagittal T2 (B), coronal STIR (C) and post-contrast sagittal (D) images show well-defined altered signal intensity area involving posteromedial aspect of body of calcaneum (arrow in B) with surrounding bone marrow oedema, showing thin rim enhancement (arrowhead) and central non-enhancing sequestrum. Cortical breach at superomedial aspect of calcaneum from which a linear enhancing sinus tract seen extending up to skin surface (dotted arrow) with adjacent inflammatory changes. Findings suggestive of chronic osteomyelitis. CBNAAT of pus discharge revealed tubercular aetiology
Necrotic areas of bone will appear low signal intensity areas on both T1- and T2-weighted images (Figs. 8, 9).
Destruction of articular cartilage and cortical bone can be visualized as defect in the hypointense cortical rim [16] (Figs. 8, 9, 10, 11, 12).
-
2.
Synovial changes Synovial inflammation can present as articular synovitis, bursal synovitis and tendon sheath synovitis.
-
Synovitis usually results in joint effusion, which is often the earliest imaging feature and appears as high signal intensity on T2WI (Figs. 8, 9, 10).
-
Synovial proliferation associated with TB arthritis is typically hypointense to intermediate signal intensity on T2WI and shows enhancement on post-contrast T1WI (Figs. 8, 9 and 12,13).
-
Granulation tissue, synovial and capsular thickening and cartilage destruction are also seen in tubercular arthritis. Articular lesions appear with low or intermediate signal intensity on T2WI [17] (Fig. 11).
-
Low signal intensity areas on T2WI correspond to fibrosis, sclerosis, new bone formation and intra-articular loose bodies [18] (Fig. 8, 9 and 11).
-
Involvement of tendons, tendon sheaths and bursae adjacent to joint result in tubercular synovitis and bursitis which appear as high signal intensity synovial effusion on T2WI with tendon sheath thickening [19] (Fig. 10 and 12).
-
-
3.
Juxta-articular soft tissue changes
Inflammation of soft tissue adjacent to joint results in cellulitis, which can be visualize as high signal intensity on T2WI with post-contrast enhancement (Figs. 8, 9, 10, 11, 12, 13, 14).
Myositis usually shows enlargement of muscles with high signal intensity on STIR and T2WI and variable post-contrast enhancement.
Granulation tissues within soft tissues show homogenous enhancement (Fig. 9) while abscesses demonstrate intermediate/high signal on T2WI with peripheral rim enhancement on post-contrast images [20] (Figs. 8 and 12).








Key imaging features
-
Unilateral joint involvement with large soft tissue abscess/collection favour tubercular ?y.
-
Late joint space reduction with end stage fibrous ankylosis are typical features of joint TB.
-
Tubercular abscesses show a smooth and thin enhancing rim at periphery while pyogenic abscesses usually show a thick and irregular peripheral rim enhancement [21].
Tubercular osteomyelitis
Presentation Pain and swelling adjacent to affected bone is commonly seen. Abscess, discharging sinus tracts may be seen in later course of disease.
Tubercular osteomyelitis of rib usually presents with chest wall cold abscess.
Location TB can affect any bone. Metaphysis is most commonly involved location for TB osteomyelitis Lesions can be solitary or multifocal.
Commonly involved sites- small bones of hands and feet and long bones of extremities.
A subtype of TB osteomyelitis is cystic tuberculosis, commonly seen in children and young adults. It usually affects the metaphysis of long bones and often skull and flat bones may be involved [22, 23].
Radiological imaging
Plain radiograph Osteomyelitis appears as diffuse osteoporosis, lytic lesion, sclerosis and periostitis. Bone sequestrum can be seen as radio-dense spicules within area of bone destruction. Osteomyelitis is often confused with malignancy on plane radiographs [10] (Figs. 15, 16).

(TB dactylitis): A 15-year-old male patient with pain, swelling right great toe. Plain radiograph of foot (A) shows of lytic destruction of 1st proximal phalanx with cortical breach and soft tissue swelling on medial aspect (oval). On MRI-Axial T1, T2 and post-contrast images (B, C and D) show altered signal intensity area appearing hypo on T1, hyper on T2WI with heterogenous post-contrast enhancement (dotted oval) and cortical breach (arrow) at proximal phalanx with soft tissue abscess and extension into 1st MTP joint. On follow-up after 14 months of ATT, radiograph foot (E) shows healing of cortical breach and resolution of lytic changes and soft tissue abscess
MR imaging features of TB osteomyelitis
Magnetic resonance imaging in tubercular osteomyelitis include T1-weighted images for better anatomical detail and delineation of medulla, cortex, periosteum and soft tissue.
Fat-suppressed and STIR sequences are better for visualization of inflammatory changes and fluid collections.
Post-contrast T1W images are obtained after administration of gadolinium-based contrast agent in suspected cases of osteomyelitis, for better characterization of abscesses and sinus tracts (Table 1).
MR imaging features of tubercular osteomyelitis are non-specific and unfortunately not useful in differentiation from pyogenic osteomyelitis.
Tubercular dactylitis affects short tubular bones of hands and feet (metacarpal, metatarsal and phalanges). Infective foci first lodge in centre and interior of short tubular bone, forming tubercular granuloma. This leads to spindle-shaped expansion of the bone (spina ventosa). Abscesses and sinus tract formation can occur secondarily leading to secondary infection and thickening of bone [25] (Fig. 16).
Tubercular tenosynovitis and bursitis
Primary tubercular tenosynovitis is rarest manifestation of osteoarticular tuberculosis. Tubercular tenosynovitis may either occur as a result of hematogenous dissemination or due to periarticular extension of tubercular arthritis (Table 2).
Clinical presentation
Common presenting feature of tubercular synovitis is carpal tunnel syndrome. This is secondary to compression of median nerve under flexor retinaculum by thick and inflamed tendon sheath. Symptoms include wrist pain, numbness and tingling sensation in fingers with decreased range of motion.
Location
Tenosynovitis- Flexor tendon sheaths of the dominant hand.
Bursitis- Trochanteric, subacromial, subgluteal and radioulnar bursae.
Tubercular synovitis can present with various forms including-
-
1.
Hygromatous stage-characterized by the presence of fluid within the tendon sheath without associated synovial thickening.
-
2.
Serofibrinous stage-characterized by thickening of flexor tendons and synovium with multiple tiny debris (rice bodies) within the synovial fluid.
-
3.
Fungoid stage-characterized by soft tissue mass involving the tendon and tendon sheath [26].
Radiological Imaging
Ultrasonography: Ultrasound is usually the primary investigation for diagnosis of tenosynovitis. It can delineate the extent and degree of involvement of the tendon and tendon sheath. Tendon and synovial thickening are predominant features seen on ultrasound with minimal effusion [27].
MR imaging features of tenosynovitis and bursitis
Tenosynovitis
Tubercular tenosynovitis mimics various non-infective inflammatory disorders such as rheumatoid arthritis, seronegative arthritis, pigmented villonodular synovitis among others (Table 3).
The characteristic MR imaging features favouring the diagnosis of tubercular aetiology include presence of low signal intensity synovial thickening on T2 WI around the flexor and extensor tendons and synovial fluid collection with low signal intensity non-enhancing foci within the tendon sheath (Fig. 11).
Additional changes such as bone erosions, osteomyelitis and median nerve encasement in wrist are also frequently seen [28].
Bursitis
Tuberculosis of bursa usually occurs in association with tubercular arthritis and osteomyelitis. It may exhibit two patterns—distension of bursa with fluid collection and multiple small abscesses [29].
On MR imaging, T2 WI images show intermediate signal intensity in area of caseous necrosis, high signal intensity correlates with effusion and low signal intensity in areas of fibrosis, sclerosis, new bone formation and intra-articular loose bodies. On T1 WI involving bursa sometimes can appear as a hyperintense lining (Fig. 8).
Conclusions
Radiologists should be aware of imaging features suggestive of osteoarticular tuberculosis and its potential mimics as MR is the emerging modality of choice for evaluation of suspected cases even in early stages of disease. This is imperative to early diagnosis and management at early-stage disease and thereby reducing complications.
Availability of data and materials
Not applicable.
Abbreviations
- TB:
-
Tuberculosis
- MRI:
-
Magnetic resonance imaging
- OATB:
-
Osteoarticular tuberculosis
- HIV/AIDS:
-
Human immunodeficiency virus/acquired immunodeficiency syndrome
- OM:
-
Osteomyelitis
References
Malaviya AN, Kotwal PP (2003) Arthritis associated with tuberculosis. Best Pract Res Clin Rheumatol 17(2):319–43
Tseng C, Huang RM, Chen KT (2014) Tuberculosis arthritis: epidemiology, diagnosis, treatment. Clin Res Foot Ankle 2:131–138
Iademarco MF, Castro KG (2003) Epidemiology of tuberculosis. Semin Respir Infect 18(4):225–240
Lupatkin H, Bräu N, Flomenberg P, Simberkoff MS (1992) Tuberculous abscesses in patients with AIDS. Clin Infect Disease 14(5):1040–1044
Moore SL, Rafii M (2001) Imaging of musculoskeletal and spinal tuberculosis. Radiol Clin N Am 39(2):329–342
Tuli SM (2002) General principles of osteoarticular tuberculosis. Clin Orthop Relat Res 398:11–19
De Backer AI, Vanhoenacker FM, Sanghvi DA (2009) Imaging features of extraaxial musculoskeletal tuberculosis. Indian J Radiol Imaging 19(3):176–86
Ansari S, Amanullah MF, Ahmad K, Rauniyar RK (2013) Pott’s spine: diagnostic imaging modalities and technology advancements. N Am J Med Sci 5(7):404
Chauhan A, Gupta BB (2007) Spinal tuberculosis. Indian Acad Clin Med 8(1):110–113
Leonard MK Jr, Blumberg HM (2017) Musculoskeletal tuberculosis. Microbio Spectrum 5(2):5–2
Jain R, Sawhney S, Berry M (1993) Computer tomography of vertebral tuberculosis: patterns of bone destruction. Clin Radiol 47(3):196–199
Agashe VM, Johari AN, Shah M, Anjum R, Romano C, Drago L, Sharma HK, Benzakour T (2020) Diagnosis of osteoarticular tuberculosis: perceptions, protocols, practices, and priorities in the endemic and non-endemic areas of the world—a waiot view. Microorganisms 8(9):1312
Ansari S, Rauniyar RK, Dhungel K, Sah PL, Chaudhary P, Ahmad K, Amanullah MF (2013) MR evaluation of spinal tuberculosis. Al Ameen J Med Sci 6(3):219–225
Griffith JF, Kumta SM, Leung PC, Cheng JC, Chow LT, Metreweli C (2002) Imaging of musculoskeletal tuberculosis: a new look at an old disease. Clin Orthop Rel Res. 398:32–9
Al-Matar MJ, Cabral DA, Petty RE (2001) Isolated tuberculous monoarthritis mimicking oligoarticular juvenile rheumatoid arthritis. J Rheumatol 28(1):204–206
Beltran J, Noto AM, McGhee RB, Freedy RM, McCalla MS (1987) Infections of the musculoskeletal system: high-field-strength MR imaging. Radiology 164(2):449–454
Suh JS, Lee JD, Cho JH, Kim MJ, Han DY, Cho NH (1996) MR imaging of tuberculous arthritis: clinical and experimental studies. J Magn Reson Imaging 6(1):185–189
Quinn SF, Murray W, Prochaska J, Cochran C, Clark R (1987) MRI appearance of disseminated osseous tuberculosis. Magn Reson Imaging 5(6):493–497
Parmar H, Shah J, Patkar D, Singrakhia M, Patankar T, Hutchinson C (2004) Tuberculous arthritis of the appendicular skeleton: MR imaging appearances. Eur J Radiol 52(3):300–309
Kim JY, Park YH, Choi KH, Park SH, Lee HY (1999) MRI of tuberculous pyomyositis. J Comput Assist Tomogr 23(3):454–457
Hong SH, Kim SM, Ahn JM, Chung HW, Shin MJ, Kang HS (2001) Tuberculous versus pyogenic arthritis: MR imaging evaluation. Radiology 218(3):848–853
Morris B, Varma R, Garg A, Awasthi M, Maheshwari M (2002) Multifocal musculoskeletal tuberculosis in children: appearances on computed tomography. Skeletal Radiol 31(1):1–8
Maiuri F, Gallicchio B, Manto A, Briganti F (1997) Spondylodiscitis: clinical and magnetic resonance diagnosis. Spine 22(15):1741–1746
Tuli SM (2010) Tuberculosis of the skeletal system (bones, joints, spine and bursal sheaths), 4[sup] th. Jaypee Brothers Medical Publishers Pvt. Ltd., New Delhi
Lee YJ, Sadigh S, Mankad K, Kapse N, Rajeswaran G (2016) The imaging of osteomyelitis. Quant Imaging Med Surg 6(2):184
Jaovisidha S, Chen C, Ryu KN, Siriwongpairat P, Pekanan P, Sartoris DJ, Resnick D (1996) Tuberculous tenosynovitis and bursitis: imaging findings in 21 cases. Radiology 201(2):507–513
Vanhoenacker FM, Sanghvi D, De Backer A (2009) Imaging features of extraaxial musculoskeletal tuberculosis. Indian J Radiol Imaging 19(03):176–186
Moore SL, Rafii M (2001) Imaging of musculoskeletal and spinal tuberculosis. Radiol Clin N Am 39(2):329–342
Hsu CY, Lu HC, Shih TT (2004) Tuberculous infection of the wrist: MRI features. Am J Roentgenol 183(3):623–628
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Dr. A.S. performed clinical evaluation and management part of all cases. Dr. R.J. analysed and interpretated all radiological imaging investigations under supervision of Dr. R.S.S. and Dr. V.C., and these are the major contributor in writing manuscript. Dr. R.K. provide data related to microbiological testing. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Informed consent
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jangid, R., Solanki, R.S., Chaudhary, V. et al. Spectrum of imaging findings in osteoarticular tuberculosis. Egypt J Radiol Nucl Med 55, 23 (2024). https://doi.org/10.1186/s43055-024-01191-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01191-5